3074
Radiomics approach in differentiating the true progression from pseudoprogression in malignant gliomas treated with concurrent radiotherapy and temozolomide chemotherapy1Department of Radiology, Henan Provincial People's Hospital, Zhengzhou, China, 2Henan Key Laboratory for Medical Imaging of Neurological Diseases, Zhengzhou, China, 3Cooperative Innovation Center of Internet Healthcare & School of Software and Applied Technology, Zhengzhou University, Zhengzhou, China
Synopsis
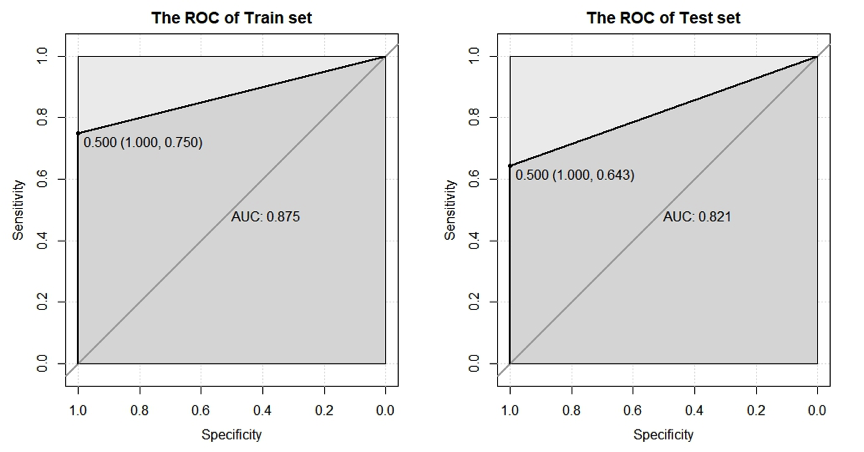
The conventional magnetic resonance imaging could not confirm the enhancing lesion in malignant gliomas after the standard postsurgical treatment is due to the ture progression or pseudoprogression. The radiomics model based on the selected magnetic resonance imaging features was established to predict the ture progression and pseudoprogression. The radiomics model yielded the AUC value of 0.875 and 0.821 for the train set and test set, respectively. The radiomics model based on the selected contrast-enhanced T1WI features is useful in differentiating the true progression from pseudoprogression in malignant gliomas treated with concurrent radiotherapy and temozolomide chemotherapy after the surgical resection.
INTRODUCTION
Glioma is the most common type of primary brain tumor in adults. The current standard therapy for the newly diagnosed malignant glioma is concurrent radiotherapy and temozolomide chemotherapy after the surgical resection.1 This treatment approach could lead to a newly developed or enlarged enhancing lesion on the follow-up contrast-enhanced T1-weighted image (T1WI). However, the conventional magnetic resonance imaging (MRI) could not confirm the enhancing lesion after therapy is due to the ture progression or pseudoprogression. Therefore, a noninvasive imaging technique that can be used to reliably differentiate the true progression from the pseudoprogression has obviously clinical implications. Radiomics is a promising field that can converts MRI data into a large number of quantitative features.2 Recently, the radiomics approach has been introduced to extend the study of gliomas beyond the conventional MRI.3 The aim of this study was to develop a radiomics model to differentiate the ture progression from pseudoprogression in the malignant gliomas treated with concurrent radiotherapy and temozolomide chemotherapy after the surgical resection.METHODS
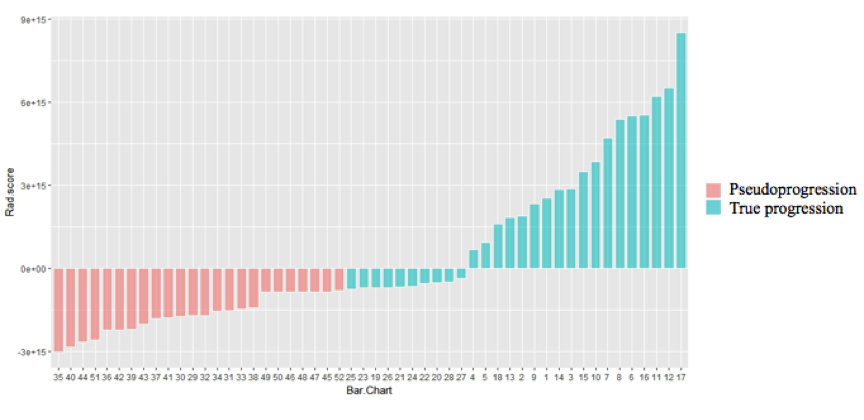
This retrospective study was approved by the local institutional review board. This study enrolled the patients with newly developed or enlarged enhancing lesion within three months of standard postsurgical treatment. The lesion due to ture progression or pseudoprogression was confirmed by the over six months follow-up MRI scans. The magnetic resonance images were collected on a 3T magnetic resonance scanner. The magnetic resonance exam included T1WI, T2WI, T2 Flair, DWI and contrast-enhanced T1WI with a single dose of gadopentetate dimeglumine. A total of 103 patients with malignant gliomas (World Health Organization III or IV grade) were included in this study. They were divided into a train cohort (n=51) and a test cohort (n=52). For each patient, the high-throughput radiomics features were extracted from the eanhancement compoment of the tumor on the contrast-enhanced T1WI. The least absolute shrinkage and selection operator was used for the dimension reduction. The radiomics model based on the selected features was established to predict the ture progression and pseudoprogression. The receiver operating characteristic curve (ROC) was used to represent the performance of the radiomics model in the train set and test set, respectively. The performance was assessed using the area under the ROC curve (AUC). The R software (version 3.4.2) was used for the statistical analysis.RESULTS
A total of 385 features including histogram, grey level co-occurrence matrix, run length matrix and grey level zone size matrix were extracted from the contrast-enhanced T1WI data. 6 significant radiomics features were selected for differentiating the ture progression from pseudoprogression in the malignant gliomas. The radiomics model based on the 6 selected features yielded the AUC value of 0.875 and 0.821 for the train set and test set, respectively.DISCUSSION
This study established a reliable radiomics model to noninvasively differentiate the true progression from pseudoprogression in the malignant gliomas. Differentiating the true progression from pseudoprogression during the early stage of standard postsurgical glioma treatment is a clinical challenge. Currently, the patient with a newly developed or enlarged enhancing lesion after therapy typically undergoes a biopsy for pathological confirmation or an over six months follow-up MRI scan . However, the biopsy is an invasive method and the follow-up MRI scan may delay the appropriate therapy. The radiomics model has the potential to predict the true progression and pseudoprogression in patients with malignant gliomas during the early stage of standard postsurgical treatment.CONCLUSION
The radiomics model based on the selected contrast-enhanced T1WI features is useful in differentiating the true progression from pseudoprogression in malignant gliomas treated with concurrent radiotherapy and temozolomide chemotherapy after the surgical resection.Acknowledgements
This research was supported by the NNSFC (81601466,81720108021, 81772009,81641168, 31470047), National Key R&D Program of China (YS2017YFGH000397), Scientific and Technological Research Project of Henan Province (182102310162) and the Key Project of Henan Medical Science and Technology Project (201501011).References
1. Sulman EP, Ismaila N, Armstrong TS, et al. Radiation therapy for glioblastoma: American Society of Clinical Oncology Clinical Practice Guideline Endorsement of the American Society for Radiation Oncology Guideline. J Clin Oncol. 2017;35(3):361-369.
2. Gillies RJ, Kinahan PE, Hricak H. Radiomics: images are more than pictures, they are data. Radiology. 2016;278(2):563-577.
3. Kickingereder P, Neuberger U, Bonekamp D, et al. Radiomic subtyping improves disease stratification beyond key molecular, clinical, and standard imaging characteristics in patients with glioblastoma. Neuro Oncol. 2018;20(6):848-857.
Figures