3072
Comparing supervised and unsupervised machine learning frameworks based upon quantitative-MRI features in differentiation between non-enhancing tumor and vasogenic edema of glioma patients and validation using histopathological ground-truthNeha Vats1, Anirban Sengupta2, Dinil Sasi3, Rakesh Kumar Gupta4, R.P. Chauhan1, Virendra Kumar Yadav3, Sumeet Agarwal5, and Anup Singh3
1NIT Kurukshetra, Kurukshetra, India, 2Centre for Biomedical Engineering, IIT Delhi, New Delhi, India, 3IIT Delhi, New Delhi, India, 4Fortis Memorial Research Institute, New Delhi, India, 5Electrical Engineering, IIT Delhi, Hauz Khas, New Delhi, India
Synopsis
The aim of this study was to compare the efficacy of unsupervised machine learning technique in differentiating non-enhancing tumor(NET) from surrounding vasogenic edema (VE) in high-grade glioma patients using T1-perfusion MRI parameters. Two unsupervised machine learning techniques, k-means clustering and Gaussian mixture model (GMM) were optimized with respect to their hyper-parameters for differentiating NET from VE and the results were compared with previously published results obtained using a supervised classifier Support Vector Machine (SVM). The results showed that SVM classifier was slightly superior to GMM and K-means clustering in differentiating NET from VE.
INTRODUCTION
The current imaging assessment of high-grade glioma (HGG) relies on the Response-Assessment-in-Neuro-Oncology (RANO)1 criteria, which suggests incorporating non-enhancing tumor component along with the enhancing component for treatment purpose. The non-contrast-enhancing lesion on FLAIR image consists of vasogenic-edema (VE) and non-enhancing tumor (NET) both of which appear similar on conventional MRI images such as FLAIR/T2-W. Quantitative dynamic-contrast-enhanced (DCE) or T1-perfusion MRI parameters (T1-PMP) have been used for differentiation between NET and VE region because of the difference in perfusion characteristics of the two regions3. Most of the studies which have used supervised learning for differentiating between NET and VE have concluded that the results should be validated with histopathology of the surgeried tissue, since there is considerable subjectivity among radiologists in delineating these regions2,3., Due to the difficulty in obtaining histopathological ground truth, most of the work on differentiation between NET and VE has used unsupervised segmentation on T1-PMP3. The objective of this study is to compare the efficacy of unsupervised segmentation against that of a previously published supervised segmentation results in differentiating between NET and VE on the same cohort4.METHODS
This study included pre-surgery and post-surgery MRI data of nine HGG patients and pre-surgery MRI data of nine Metastasis-patients. MRI protocol for this study included acquiring conventional images, data for pre-contrast T1 maps, and DCE-MRI data of brain. T1-PMP were computed from DCE-MRI data using in-house built Matlab based software. Normalized cerebral-blood-flow (CBF NWM), leakage corrected cerebral-blood-volume (CBVcorr NWM), and fraction of blood-plasma-volume (Vp) were used for differentiation as the other parameters such as Ktrans, Ve and Kep are not applicable in NET and vasogenic edema region. The ground truth for NET and vasogenic edema was obtained using a previously published method on the same cohort4. Histopathological analysis of surgeried tissue of glioma patients was done to validate the proposed ground truth of NET region. Two unsupervised clustering methods were used to differentiate between NET and VE; one is a hard clustering method (K-means) and the other is a soft clustering method which is Gaussian-Mixture-Model (GMM). GMM was optimized based on the type of ‘covariance matrix’ of the data, which can be either full or diagonal. K-means algorithm was optimized based on different distance measurement techniques such as ‘cityblock’, ‘euclidean’, ‘cosine’ and ‘correlation’. Optimization of GMM and K-means clustering was done based on misclassification error % obtained with respect to the proposed ground truth. The results of optimized unsupervised learning methods were compared with the results of a supervised classifier Support-Vector Machine (SVM) whose results have been published previously on the same cohort4.RESULTS
The histogram analysis results in Figure1 showed that NET has higher values of CBF NWM and CBVcorr NWM compared to VE although there is some overlap among the two regions. Vp showed least differentiation between the two regions among the different features. The data distribution in the two clusters is slightly different between two unsupervised techniques as more data is allocated to vasogenic edema in k-means as compared to GMM (Figure2). The hyper-parameters covariance type-‘full’ and shared covariance- ‘false’ provided best results for GMM as shown in Table2. The distance measure ‘cityblock’ provided least misclassification error % in case of k-means (Table3). The results of optimal GMM performed slightly better than optimal K-means classifier as per the misclassification error (13.04 % against 14.33 %). However, the misclassification error of GMM was slightly more compared to the results of supervised SVM classifier which had 8.4 % misclassification error on combined glioma and metastasis patients (Table1).DISCUSSION
The low misclassification error obtained using both the unsupervised methods suggest that it is feasible to distinguish NET and VE based on perfusion parameters as they have different perfusion characteristics. The slightly better results obtained using soft clustering technique GMM over hard clustering technique K-Means is probably because instead of finding the centroids as in K-means, GMM finds gaussians that best fit the data. The SVM classifier which has good generalization power because of using a non-linear kernel and regularization parameter supersedes the performance of GMM which pre-assumes that the data distribution is gaussian in nature. The supervised classifier is able to develop a model which takes into account the particular peculiarities of the data distribution, without pre-assuming any particular nature of the data.CONCLUSION
The low misclassifcation error % obtained using unsupervised learning validates the usage of unsupervised learning in previous studies aimed at differentiating NET from VE. However, results suggests that using supervised learning can further improve the results over unsupervised learning.Acknowledgements
The Authors acknowledge technical support of Philips India Limited in MRI data acquisition. This work was supported by Science and EngineeringResearchBoard (IN) (YSS/2014/000092).References
[1] David N. Louis, Arie Perry, Guido Reifenberger, Andreas von Deimling, Dominique Figarella-Branger, Webster K. Cavenee, Hiroko Ohgaki, Otmar D. Wiestler, Paul Kleihues, David W. Ellison, The 2016 world health organization classification of tumors of the central nervous system: a summary, Acta Neuropathol. 131 (2016) 803–820, https://doi.org/10.1007/s00401-016-1545-1. [2] Blumenthal DT, Artzi M, Liberman G, Bokstein F, Aizenstein O, Ben Bashat D. Classification of High-Grade Glioma into Tumor and Nontumor Components Using Support Vector Machine, Am J Neuroradiol. 2017 May;38(5):908-914. doi: 10.3174/ajnr.A5127. [3] Artzi M, Bokstein F, Blumenthal DT, Aizenstein O, Liberman G, Corn BW, Ben Bashat D. Differentiation between vasogenic-edema versus tumor-infiltrative area in patients with glioblastoma during bevacizumab therapy: a longitudinal MRI study. Eur J Radiol. 2014 Jul;83(7):1250-1256. doi: 10.1016/j.ejrad.2014.03.026. [4] Anirban Sengupta, Sumeet Agarwal, Pradeep Kumar Gupta, Sunita Ahlawat, Rana Patir, Rakesh Kumar Gupta, Anup Singh , On differentiation between vasogenic edema and non-enhancing tumor in high-grade glioma patients using a support vector machine classifier basedupon pre and post-surgery MRI images. https://doi.org/10.1016/j.ejrad.2018.07.018Figures
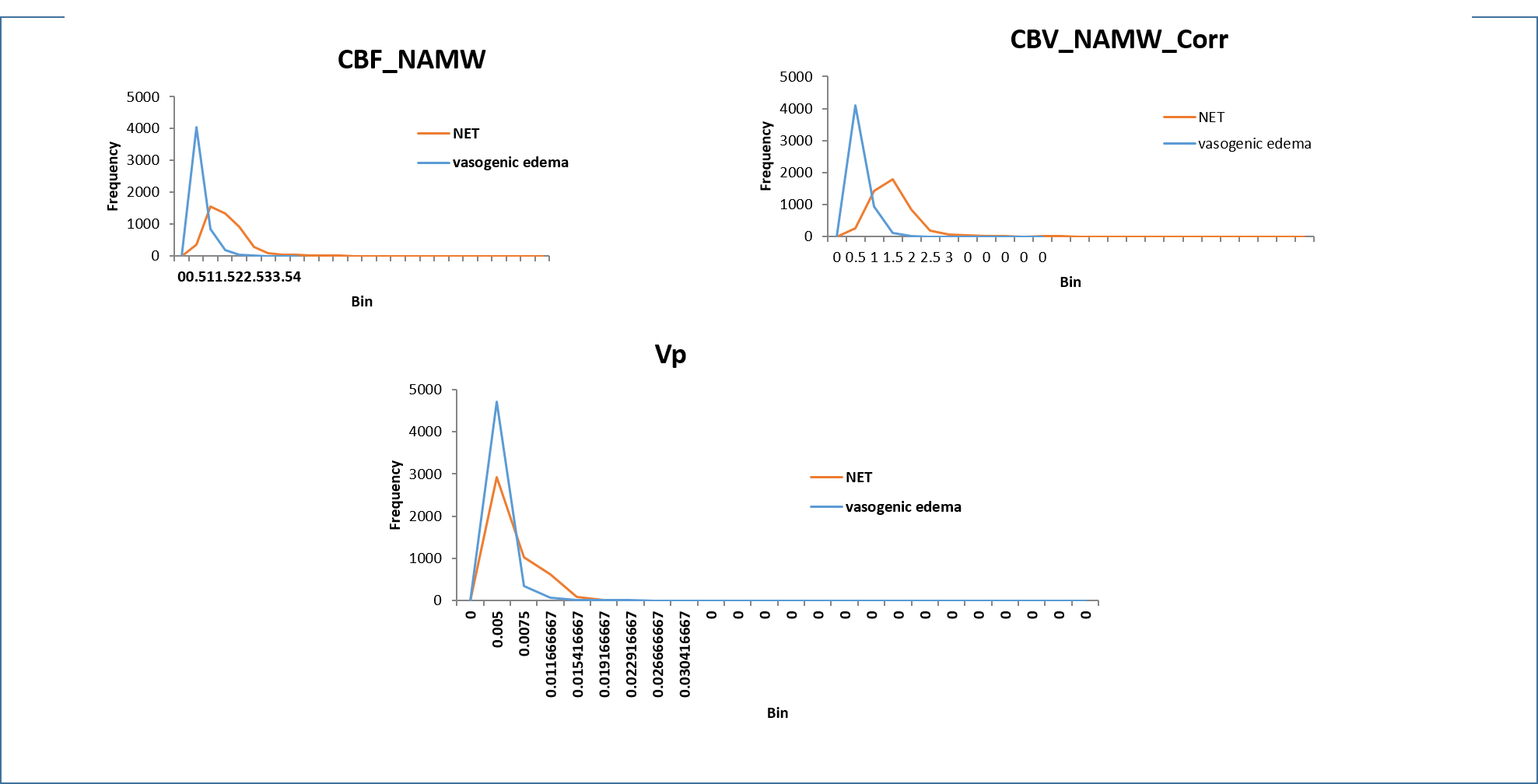
Figure1:
Figure shows the histogram distribution of T1 perfusion
parameters
CBF
NWM, CBVcorr
NWM
and Vp
in the
non-enhancing tumor region and vasogenic
edema .
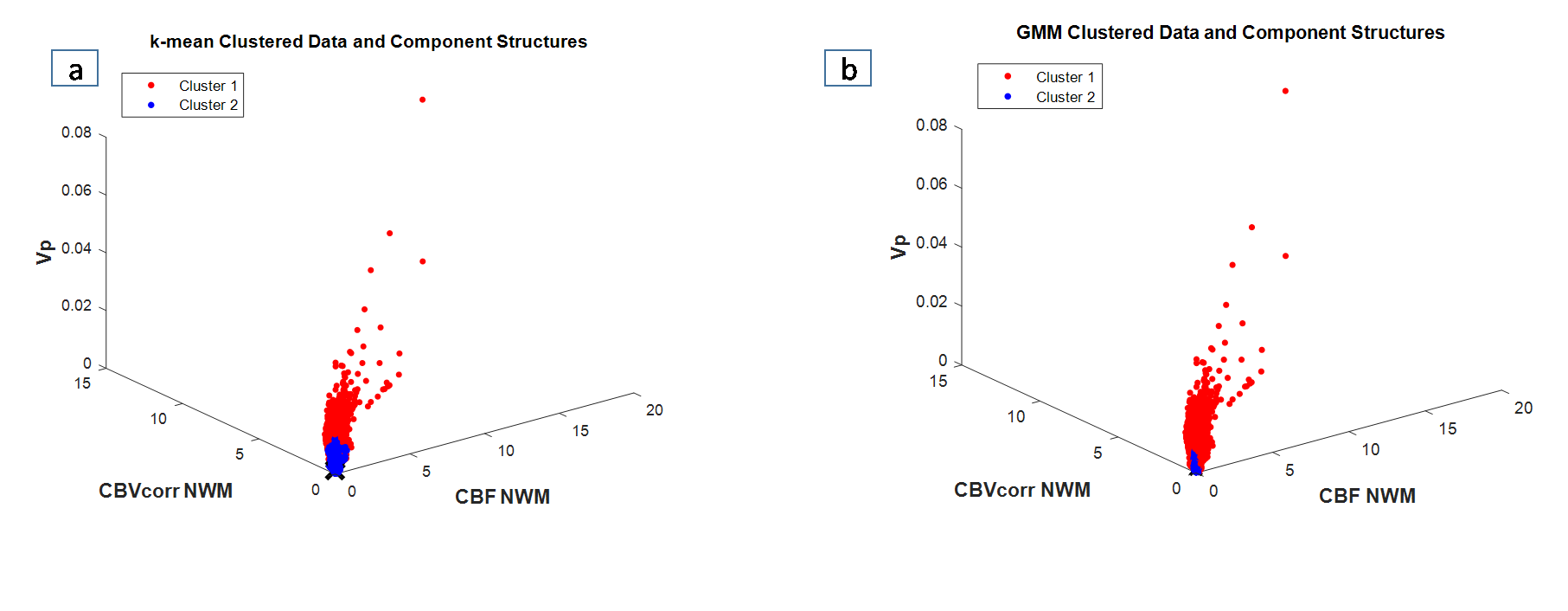
Figure2:
Plot(a)
and plot(b) shows the distribution of data in 2 clusters
using k-means clustering and GMM. Cluster1
represents non-enhancing tumor and cluster2 represents vasogenic
edema region.
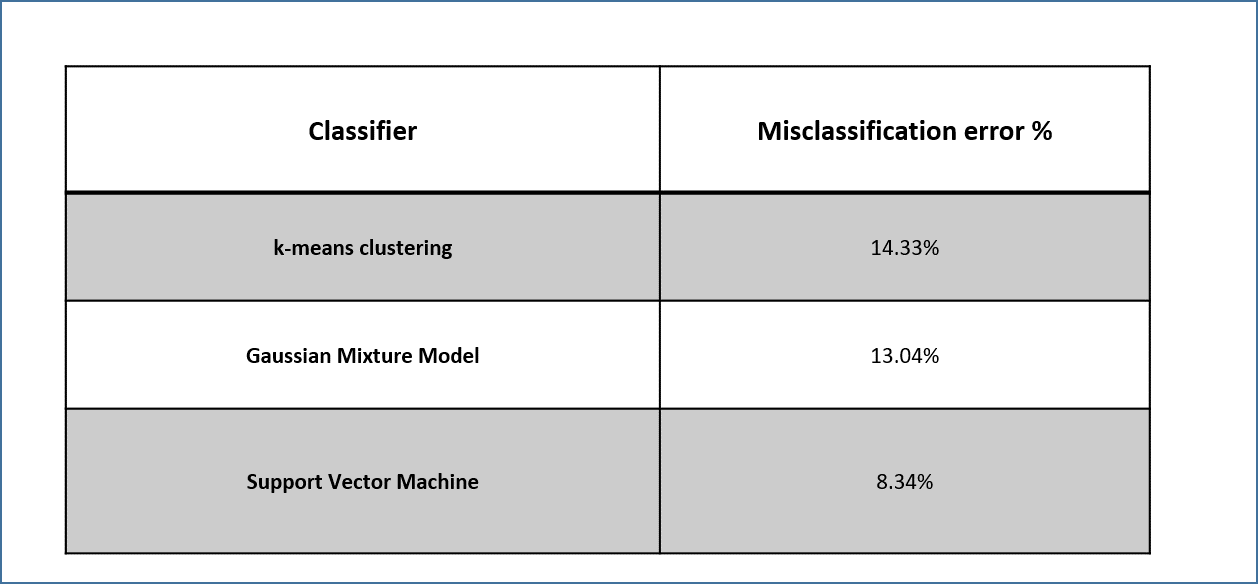
TABLE
1: Table
represents misclassification error % in differentiating non-enhancing tumor
from vasogenic
edema obtained using supervised and unsupervised machine learning techniques.
Result shows that SVM has the least misclassification error %.
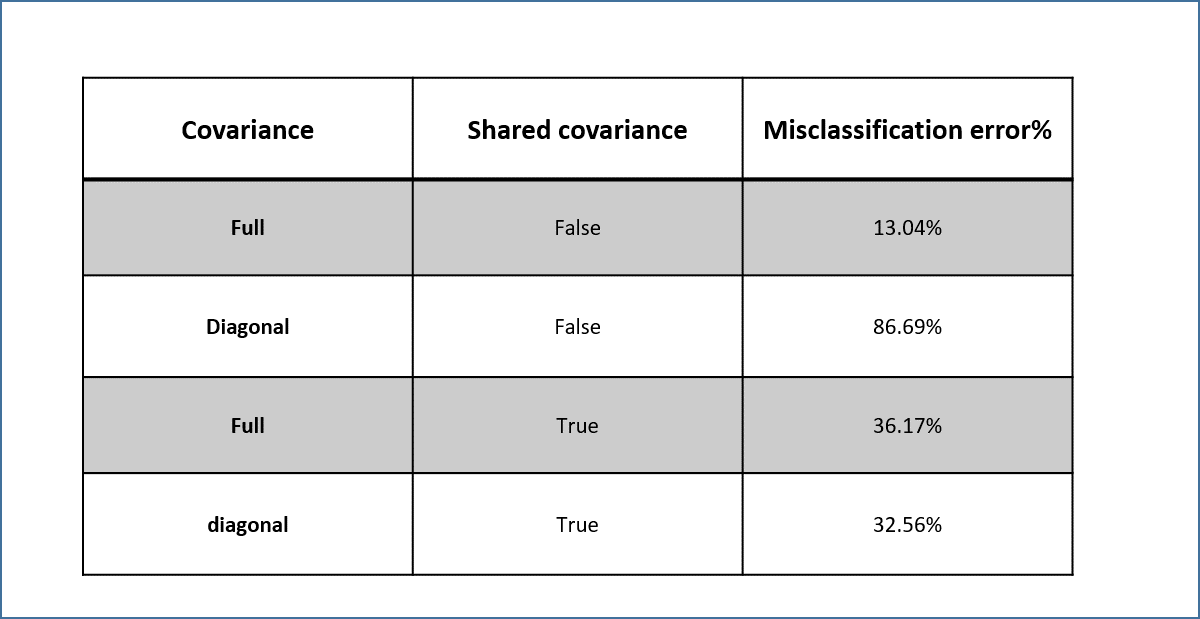
TABLE
2: Table
shows comparison of misclassification error% obtained using various
hyper-parameter combinations in GMM. The best results are obtained for the
hyper-parameters: covariance as ’full’ and shared covariance as ‘false’.
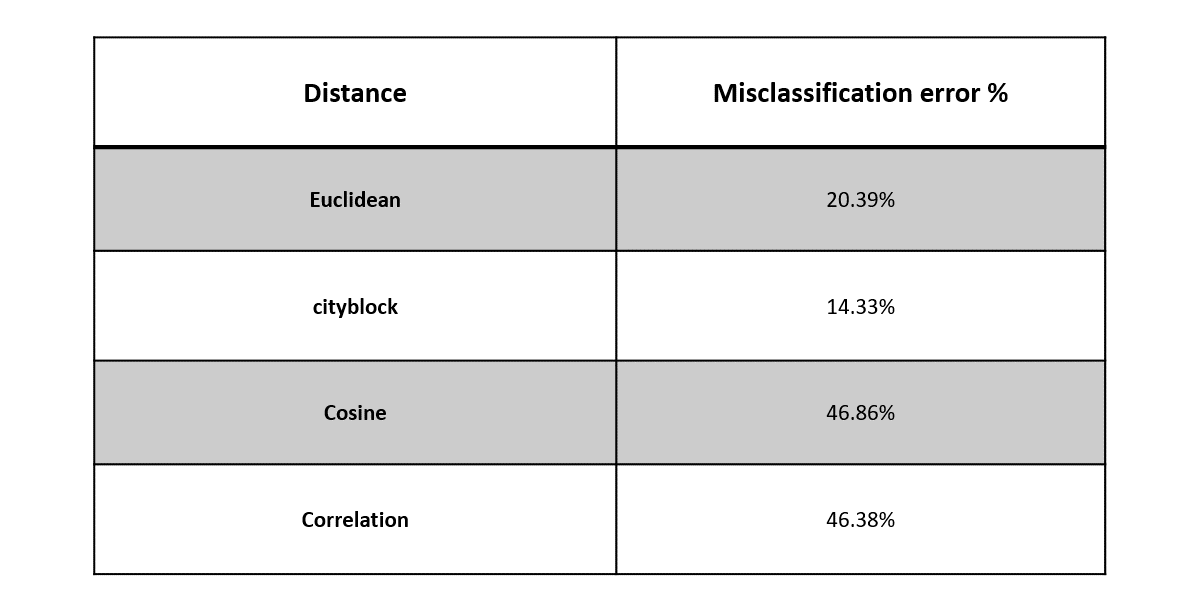
TABLE
3: Table
shows comparison of misclassification error % obtained using different distance
measurement techniques in k-means clustering. The best results are obtained
using ‘cityblock’
as a distance measure.