3067
Conventional MR-based machine learning for distinguishing brain glioma and solitary metastasis1The first affiliated Hospital of XI'AN Jiaotong University, XI'AN, China, 2Xi’an Jiaotong University, XI'AN, China
Synopsis
Differentiation of brain glioma and solitary metastasis is clinically crucial for prescribing the patients’ management and assessing the prognosis. However, indistinguishable signs between two tumors on conventional MRI always embarrass the radiologists and thus lead to high misdiagnosis rate. To address such issue, series of MR features like grey level co-occurrence matrix, histograms of oriented gradient, shape and etc. were first extracted to detail the tumors’ histologic and morphologic characteristics. Then, a gradient-boosting machine learning approach was employed to distinguish the two tumors by the MR features. A good performance with area under receiver operating characteristic curve 0.80, sensitivity 85% and specificity 78% was obtained, suggesting the potential role of our approach in identifying brain glioma and solitary metastasis.
Introduction
Glioma and brain metastasis account for more than half of all brain malignant tumors1. Differentiation of the two neoplasms is clinically crucial for prescribing the patients’ management and assessing the prognosis2. However, indistinguishable signs between two tumors on conventional MRI always embarrass the radiologists and thus lead to high misdiagnosis rate. Previous studies reported that diagnostic ability of conventional MRI was limited with an area under receiver operating characteristic curve range of 0.65~0.753-6. To address such issue, we analyzed and extracted series of MR features to detail the tumors’ histologic and morphologic characteristics. In addition, a gradient-boosting (GDBT) machine learning was used to serve for distinguishing the two tumors by the above MR features.Methods
From May 2015 to May 2018, 119 patients who underwent T2 weighted image (T2WI) and T1 contrast enhanced (T1-CE) were retrospectively enrolled in this study. Inclusion criteria: 1) pathologically confirmed newly diagnosed gliomas; 2) pathologically or follow-up confirmed newly diagnosed brain metastasis; 3) availability of diagnostic-quality preoperative MR images with obvious brain tumor. Exclusion criteria: 1) Incomplete MR data; 2) MRI examination interval between plain and enhanced scan was more than 7 days.
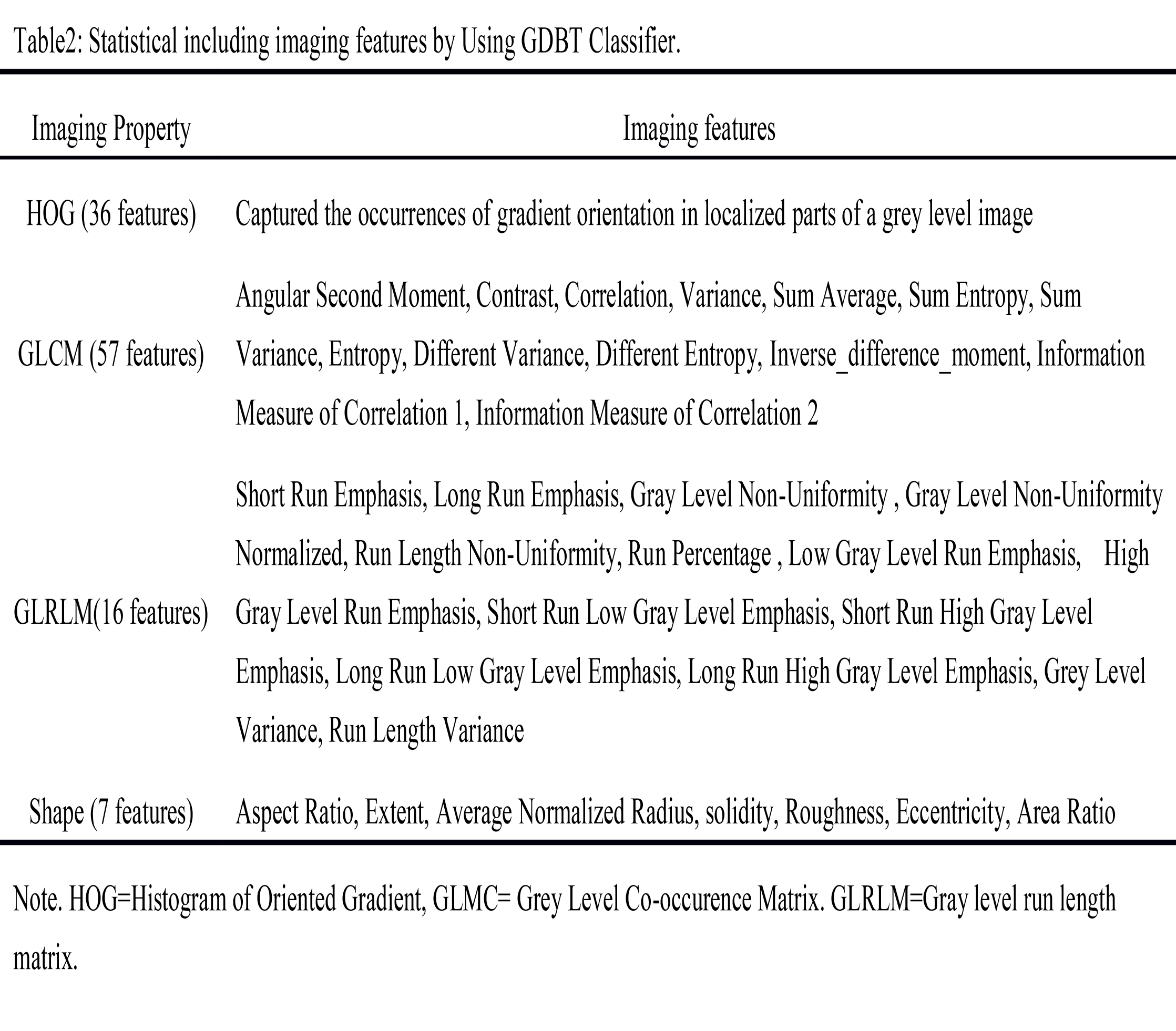
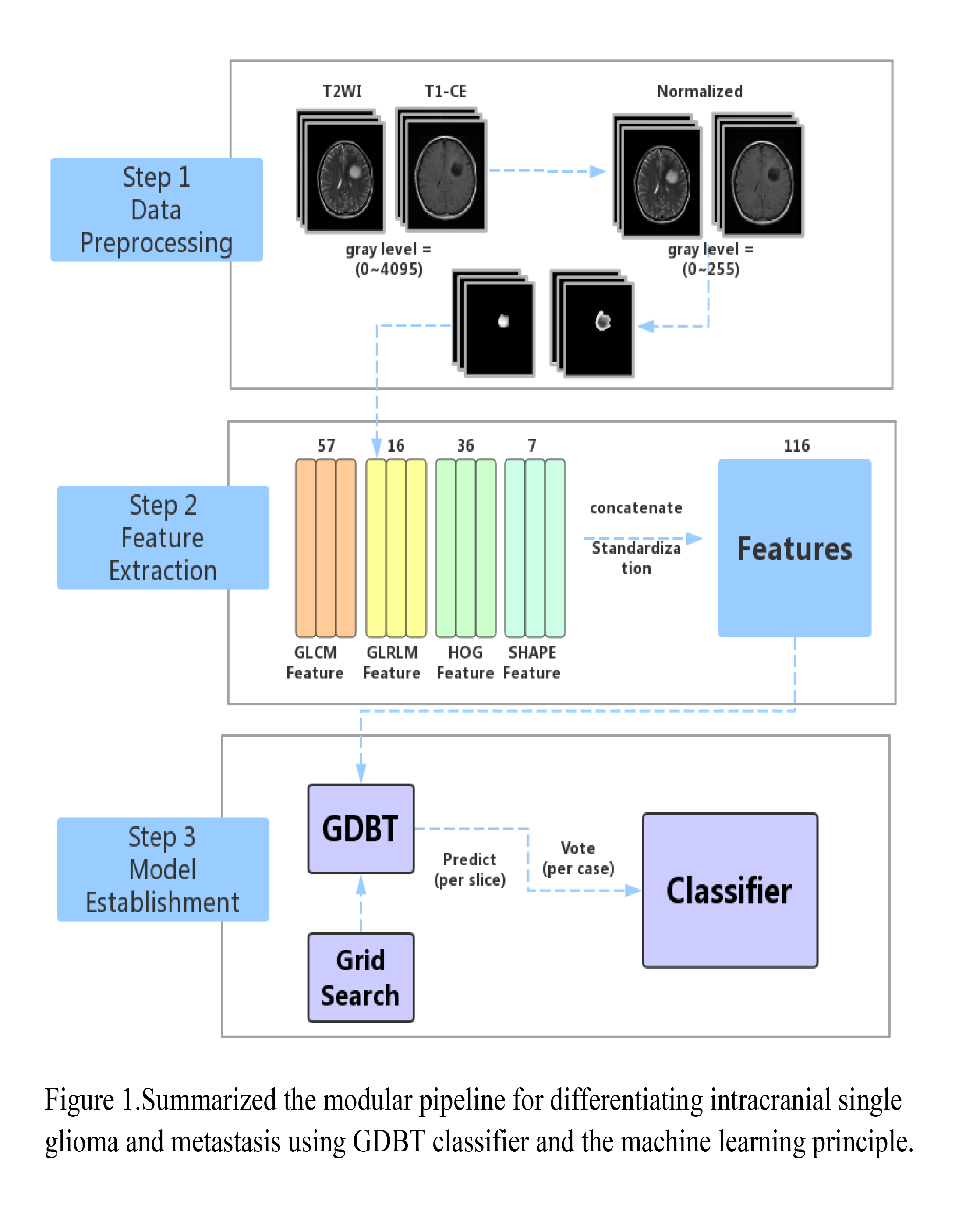
Figure 1 depicted the pipeline of data processing. The region of interest (ROI) of tumor segmentation was manually performed using the ITK-SNAP software (www.itk-snap.org) based on T2WI and T1-CE images. 116 MR features including 57 grey level co-occurrence matrix (GLCM), 36 histogram of oriented gradient (HOG), 16 gray level run length matrix (GLRLM) and 7 shape features were extracted from ROI on each slice (Table 2). Based on the extracted features, two GDBT machine learning models were separately established for T2WI and T1-CE in distinguishing brain glioma and solitary metastasis. A 5-fold cross-validation was used to evaluate the machine learning model efficiency and the area under receiver operating characteristic (ROC) curve (AUC) was used to evaluate the diagnostic performance. In addition, a binary logistic regression was employed to combine the ROCs of T1-CE and T2WI. Analyses were performed with python software (Version 3.6, Python Software Foundation).
Further, a comparison of diagnostic performance between the machine learning and radiologist were performed. Five radiologists with 3 to 5 years of experience reviewed all MR images and made their diagnosis of glioma or metastatic tumor according to tumor location, size, enhanced degree, edema degree without any clinical and pathological information. AUC was used to evaluate the radiologists’ diagnostic performance.
Results
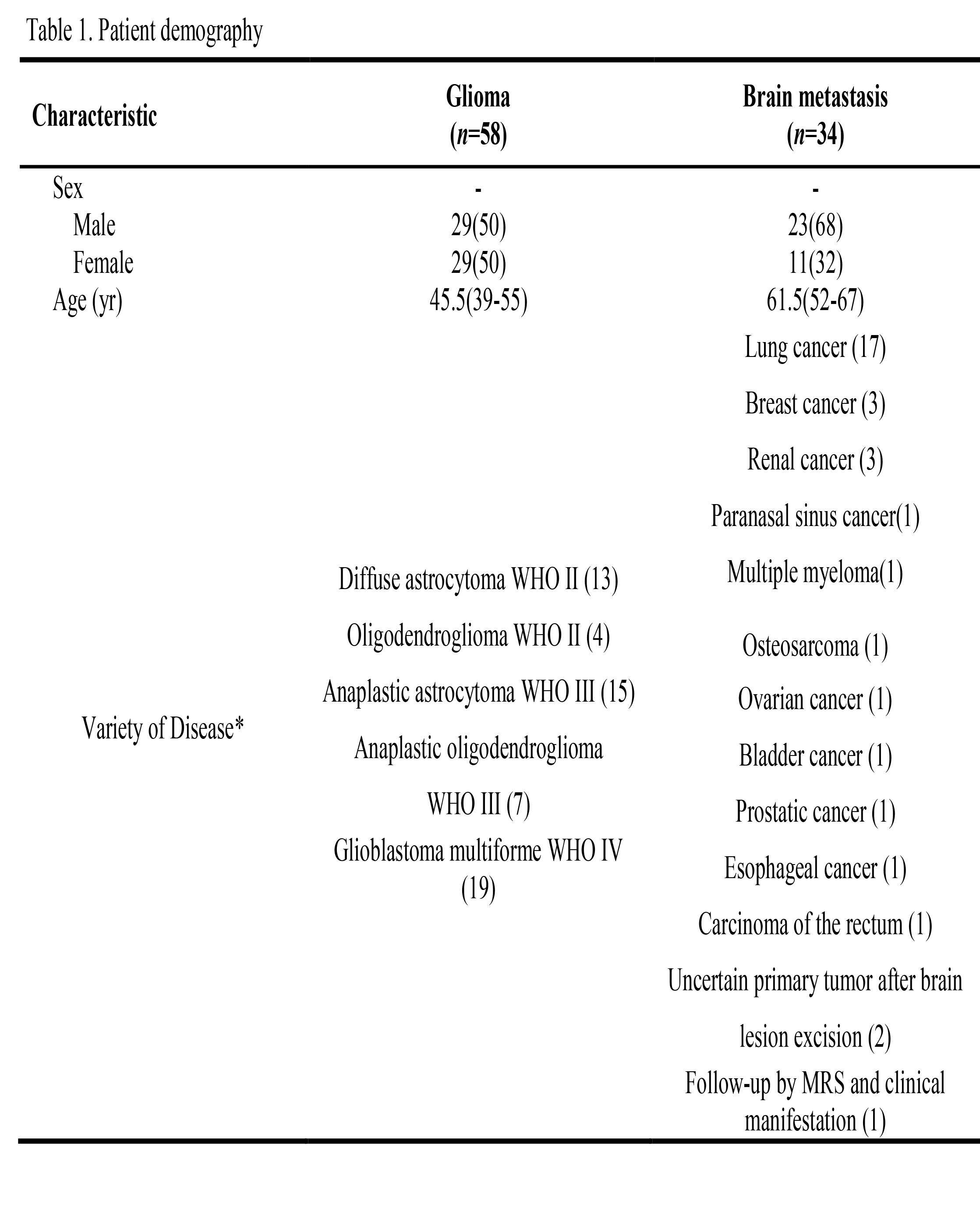
The detailed clinical characteristics of 92 patients (58 gliomas and 34 brain metastasis) were summarized in Table1. No significant difference was found between two tumors for sex (P=0.23), while there was significant difference for age (P<0.001).
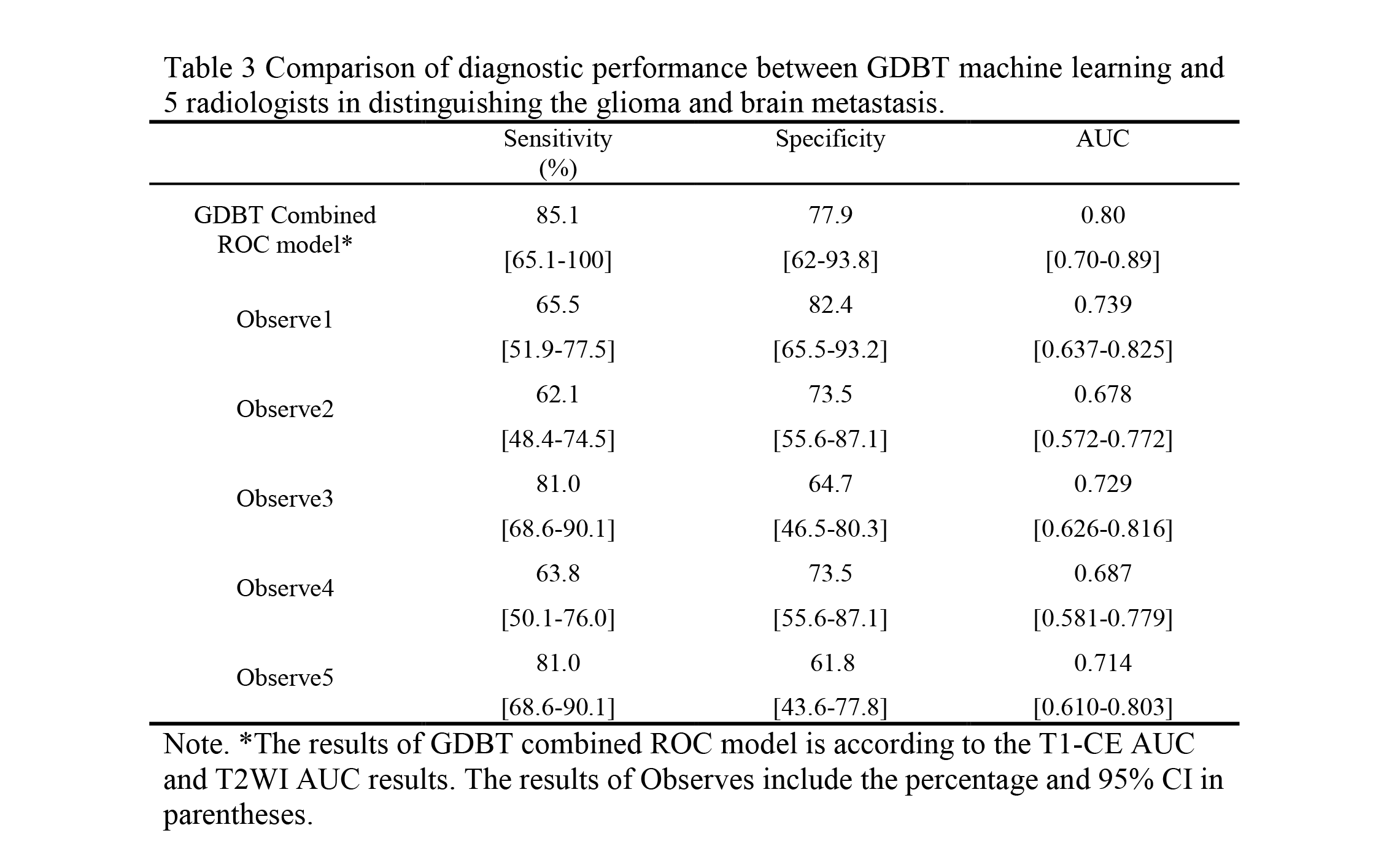
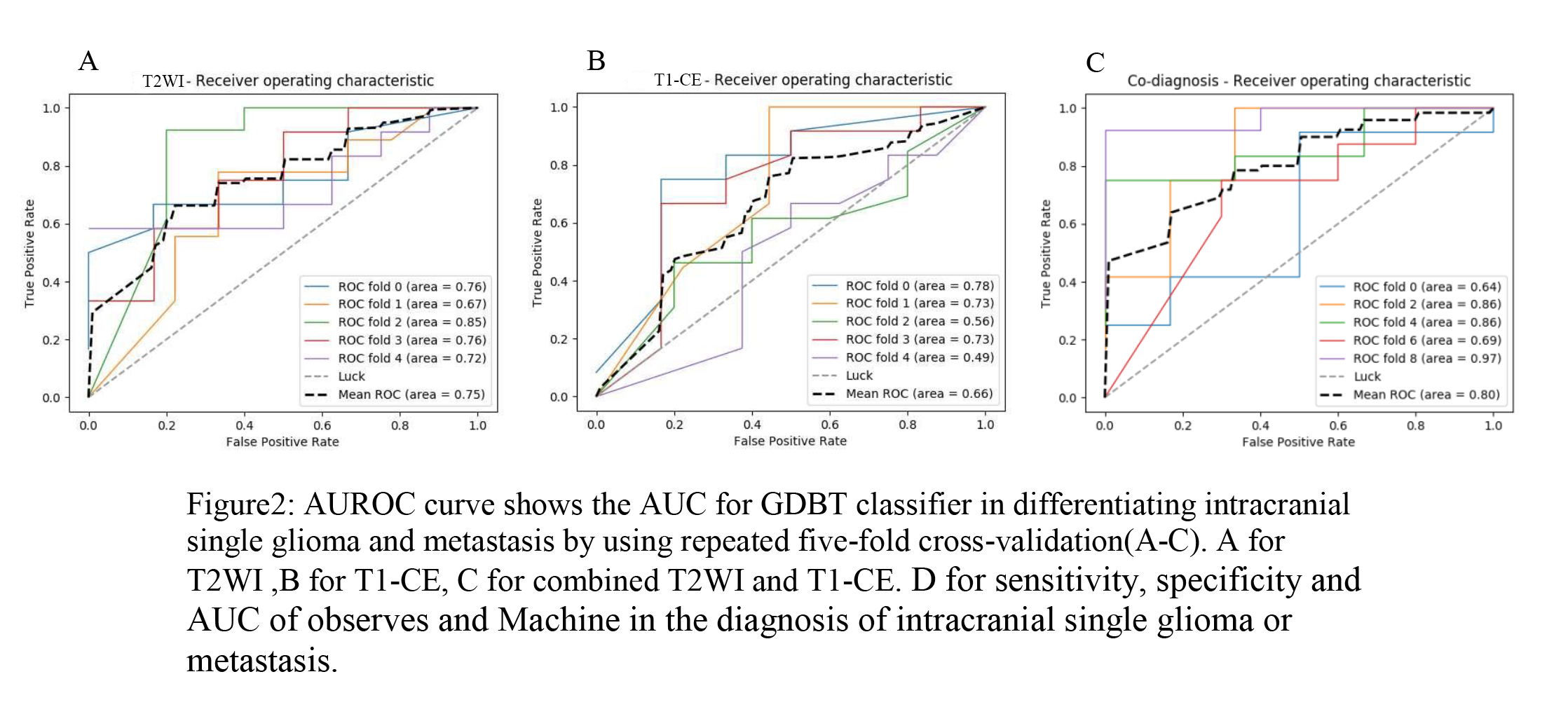
Our results indicated that the sensitivity, specificity, AUC for T2WI features were 70.7%, 80.2% and 0.75; those for T1-CE were 70.9%, 70.4% and 0.66; those for combining T2WI and T1-CE were 85%, 78%, 0.80. (Figure 2).
The mean sensitivity, specificity and AUC of 5 radiologists were 70.68%, 71.18%, 0.72, respectively (Table 3).
Discussion
In this study, based on 116 MR features detailing tumor pathology, we performed a GDBT machine learning model for distinguishing the glioma from brain solitary metastasis. In contrast to previous methods and radiologists, our machine learning approach presented remarkably better diagnostic performance. This suggest the potential role of this method in clinical tumor diagnosis.
Different from previous simple features like mean signal value and tumor size, this study employed the 116 textual and shape features that could reflect the tumor heterogeneity and its underlying pathophysiologic information. It may be such detailed features that led to better performance in distinguishing the two tumors. Besides, a GDBT machine learning model was selected as classifier due to its powerful integration of image features. In addition, previous study also demonstrated GDBT showed wide practicability in a range of fields. By using GDBT model, we indeed obtained good performance in classifying the glioma and brain metastasis.
Conclusion
This study developed a conventional MR features-based machine learning model to noninvasively distinguish the glioma and brain solitary metastasis, which may provide an alternative way to assist the radiologists’ burdensome works in clinical practice.Acknowledgements
This study was supported by the National Key Research and Development Program of China (2016YFC0100300), National Natural Science Foundation of China (No. 81471631, 81771810 and 51706178), the 2011 New Century Excellent Talent Support Plan of the Ministry of Education, China (NCET-11-0438) and the Clinical Research Award of the First Affiliated Hospital of Xi’an Jiaotong University (No. XJTU1AF-CRF-2015-004).References
[1] Chen L, Zou X, Wang Y, et al. Central nervous system tumors: a single center pathology review of 34,140 cases over 60 years. BMC clinical pathology, 2013, 13(1): 14.
[2] Giese A, Westphal M. Treatment of malignant glioma: a problem beyond the margins of resection. Journal of cancer research and clinical oncology, 2001, 127(4): 217-225.
[3] Tang, Y. M., S. Ngai, and S. Stuckey. The solitary enhancing cerebral lesion: can FLAIR aid the differentiation between glioma and metastasis?. American journal of neuroradiology, 2006,27(3): 609-611.
[4] G Yang, TL Jones, FA Howe et al. Morphometric model for discrimination between glioblastoma multiforme and solitary metastasis using three‐dimensional shape analysis. Magnetic Resonance in Medicine,2016, 75(6): 2505-2516.
[5] MH Maurer, M Synowitz, H Badakshi et al. Glioblastoma multiforme versus solitary supratentorial brain metastasis: differentiation based on morphology and magnetic resonance signal characteristics. Fortschr Röntgenstr, 2013,185(3): 235–240.
[6] N Mouthuy, G Cosnard, J Abarca-Quinones et al. Multiparametric magnetic resonance imaging to differentiate high-grade gliomas and brain metastases.Journal of Neuroradiology,2012,39(5), 301-307.
[7] Natekin A, Knoll A. Gradient boosting machines, a tutorial. Frontiers in neurorobotics, 2013, 7:21.
[8] Tian Q, Yan L F, Zhang X, et al. Radiomics Strategy for Glioma Grading Using Texture Features From Multiparametric MRI; Scientific reports, 2017, 7(1): 5467.
Figures