3055
Reduced Brain Volume and Integrity in Alzheimer’s HFEH63D CarriersCarson J Purnell1, Jian-Li Wang1, Qing X Yang1, James R Connor2, and Mark D Meadowcroft1,2
1Radiology, The Pennsylvania State University - College of Medicine, Hershey, PA, United States, 2Neurosurgery, The Pennsylvania State University - College of Medicine, Hershey, PA, United States
Synopsis
The data demonstrate that the HFEH63D polymorphism reduces apparent brain integrity in AD carriers. AD-HFEH63D carriers have reduced white matter integrity, increased cortical loss, increased amyloid-beta (Aβ) deposition, and an accelerated disease course trajectory compared to HFEWT carriers in regions susceptible to AD pathology. This work helps decipher how HFE mutations affect AD trajectory, regional susceptibility to AD pathology, brain aging integrity, and cognitive decline.
Introduction
Data suggest that subpopulations of white and gray matter brain tissue have varying degrees of susceptibility to Alzheimer’s pathological insults, leading to cell dysfunction or death. Our group has outlined a single nucleotide polymorphism (SNP) in the HFE gene sequence which is involved in aging brain integrity 1,2. The H63D missense mutation3 (HFEH63D, rs1799945) regionally reduces white matter integrity in cognitively normal carriers2. The HFE-H63D gene variant is a highly prevalent single nucleotide polymorphism (SNP) with approximately 16% global penetrance. Our preliminary analysis demonstrated that the HFEH63D mutation has a marked effect on white matter integrity in AD patients. This work aims to determine if the HFEH63D genotype acts as a disease modifier and its relationship to regional brain pathology and susceptibility in AD course.Methods
Data from 432 subjects (305 AD/MCI) from the ADNI cohort were used in this study, selected based on the presence of genetic sequencing data. Anatomical T1, diffusion, FDG-PET, and AV-45 PET images were downloaded and pre-processed using AFNI. T1 images were additionally processed using the DARTEL VBM toolbox in SPM8 to investigate volumetric differences between groups. Subjects were separated into six groups (AD, MCI, and CN) based on cognitive status and HFEH63D genotype, and statistical analyses were carried out using SPM8. Linear mixed effect (LME) modeling was used to determine linear trends in the data with 3dLME statistical R coding within AFNI.Results
Cortical volume loss is observed in HFEH63D carrier AD patients compared to AD-HFEWT, indicating a negative interaction effect between HFEH63D and AD (Fig. 1). Regions with decreased volume include the insula, cingulate, inferior and orbital frontal gyri, caudate, and a large extent of the temporal lobe. LME modeling of cortical volume demonstrated an increased linear trend in AD HFEH63D carriers compared to HFEWT (Fig. 2). AD HFEH63D carriers had an increase in (a) gray and (b) white matter mean diffusion throughout the brain (Fig. 3). AV-45 measures demonstrates an increase in amyloid burden in AD HFEH63D carriers in regions known to be effected by early amyloid pathology (Fig. 4). AD HFEH63D carriers demonstrated a decrease cortical metabolism in known AD effected regions and hyper-metabolism in temporal structures (Fig. 5).Discussion
The absolute voxel-based morphometry analysis illustrated regions with a less relative cortical volume in the AD HFEH63D carriers. The regions outlined are known to have early and progressive Aβ and Tau AD pathology. The LME model demonstrated that AD HFEH63D carriers had an increase linear trend in cortical volume loss. The increase in mean diffusion in the AD HFEH63D carriers in both cortical gray and white matter in indicative of a general loss of brain cellularity and integrity in regions known to be effected in AD. HFEH63D carriers demonstrate an increase in amyloid burden and altered metabolism.Conclusion
The data demonstrate that AD-HFEH63D carriers have reduced white matter integrity, increased cortical loss, increased amyloid-beta (Aβ) deposition, and an accelerated disease course trajectory compared to HFEWT carriers in regions susceptible to AD pathology. The HFEH63D polymorphism reduces apparent brain integrity in AD carriers, data which is congruent with our work in cognitively normal HFEH63D subjects. Future work will interrogate the cellular interaction between the HFE polymorphism and neurodegenerative disease.Acknowledgements
No acknowledgement found.References
1. Meadowcroft MD, Wang J, Purnell CJ, et al. Reduced Cerebral White Matter Integrity Assessed by DTI in Cognitively Normal H63D-HFE Polymorphism Carriers. J Neuroimaging. Jan 2018;28(1):126-133. 2. Meadowcroft MD, Wang J, Purnell CJ, et al. Reduced white matter MRI transverse relaxation rate in cognitively normal H63D-HFE human carriers and H67D-HFE mice. Brain Imaging Behav. Dec 11 2016;10(4):1231-1242. 3. Feder JN, Gnirke A, Thomas W, et al. A novel MHC class I-like gene is mutated in patients with hereditary haemochromatosis. Nat Genet. Aug 1996;13(4):399-408.Figures
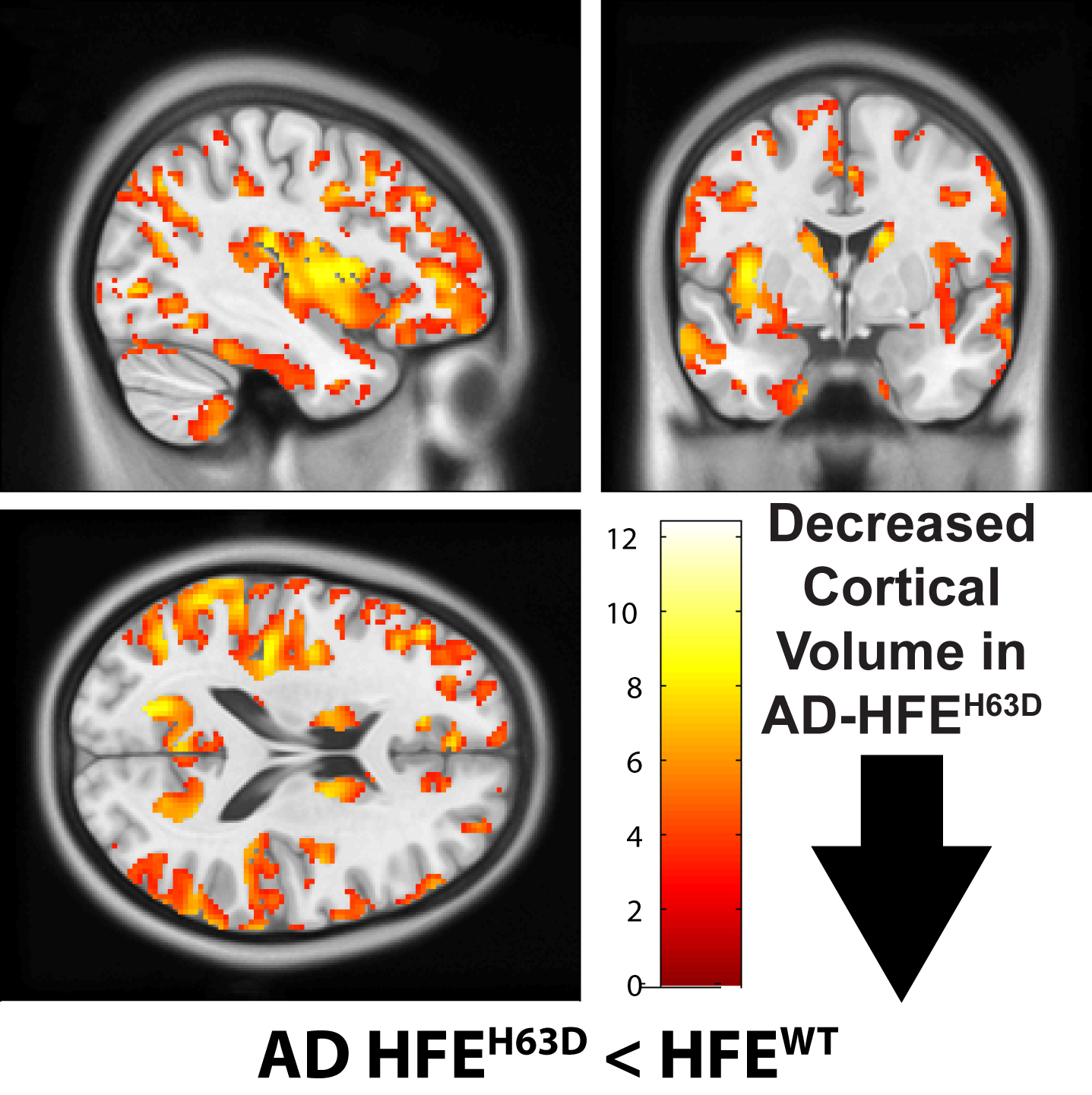
Figure
1 – Cortical volume loss is
observed in HFEH63D carrier AD patients compared to AD-HFEWT,
indicating a negative interaction effect between HFEH63D and AD. p<0.005,
50 voxel threshold.
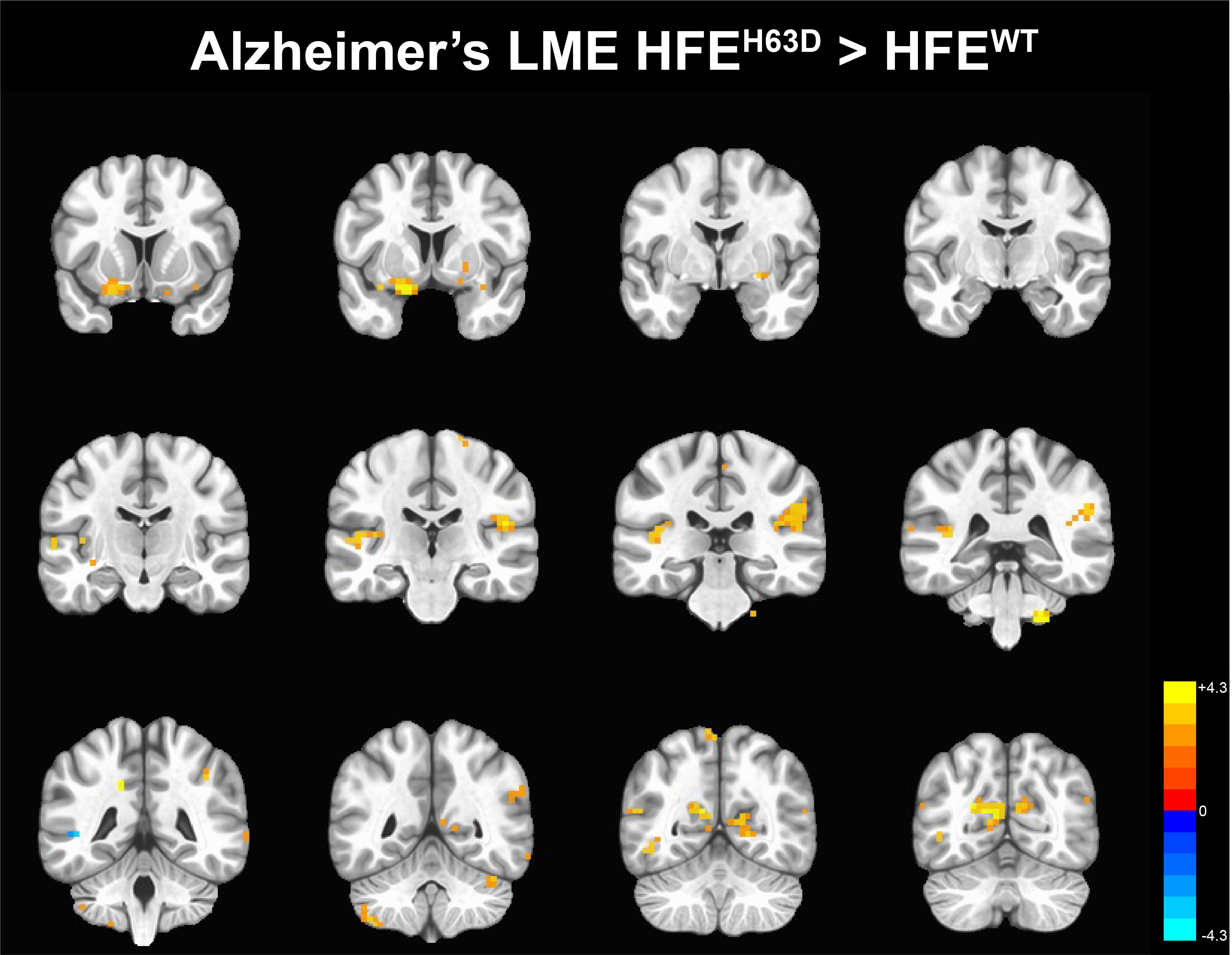
Figure
2 – Linear mixed effect modeling of volumetric loss in HFEH63D AD
carriers. The data demonstrate that AD
H63D carriers have an increased linear trend in cortical loss compared to HFEWT
carriers. p<0.01, 50 voxel threshold.
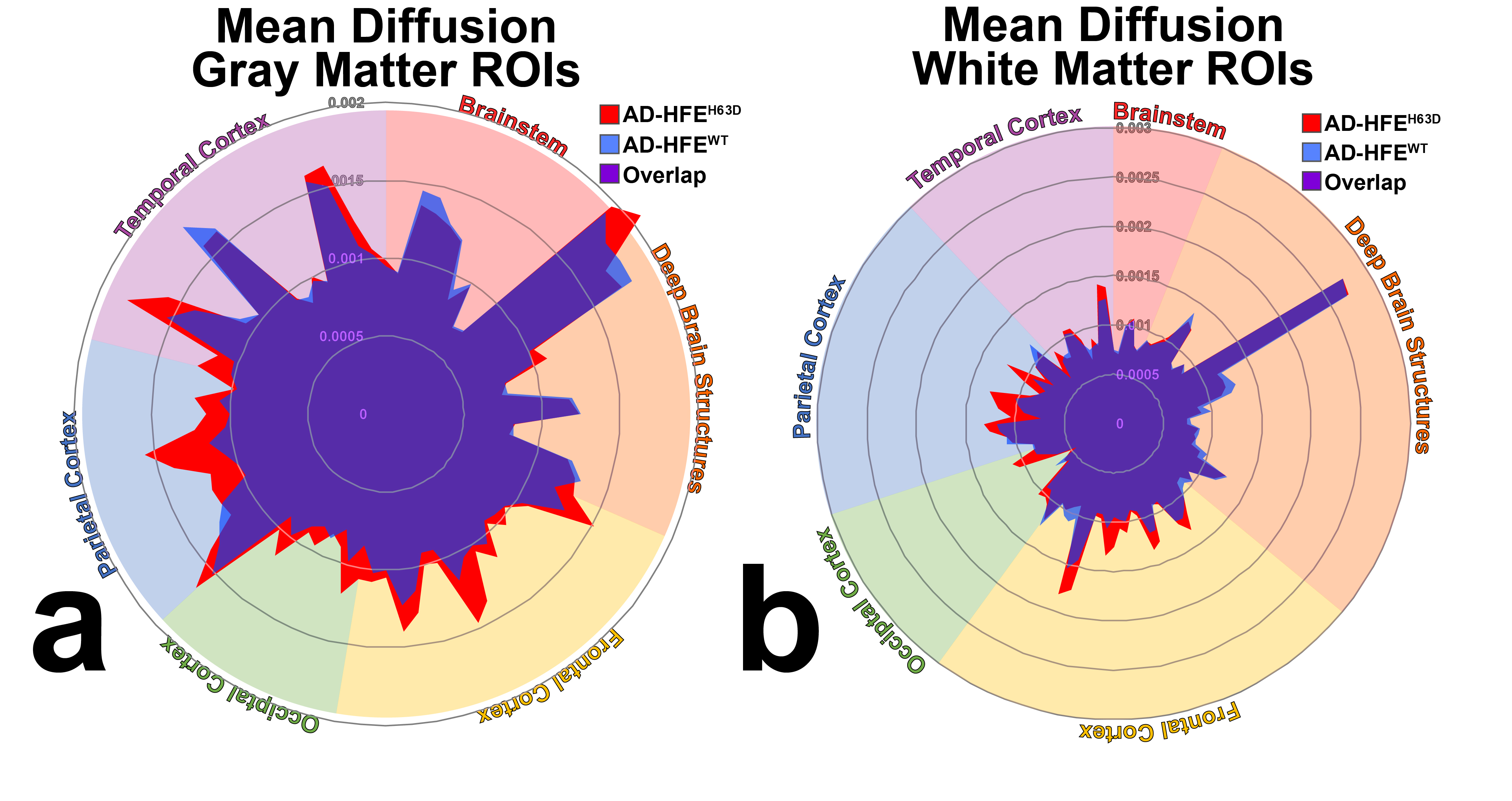
Figure
3 – Radial splatterplot of a) gray and b) white matter mean diffusion in HFEWT
and HFEH63D AD carriers. AD-HFEH63D patients have
multiple regions throughout the brain with increased MD, indicative of reduced
brain integrity.
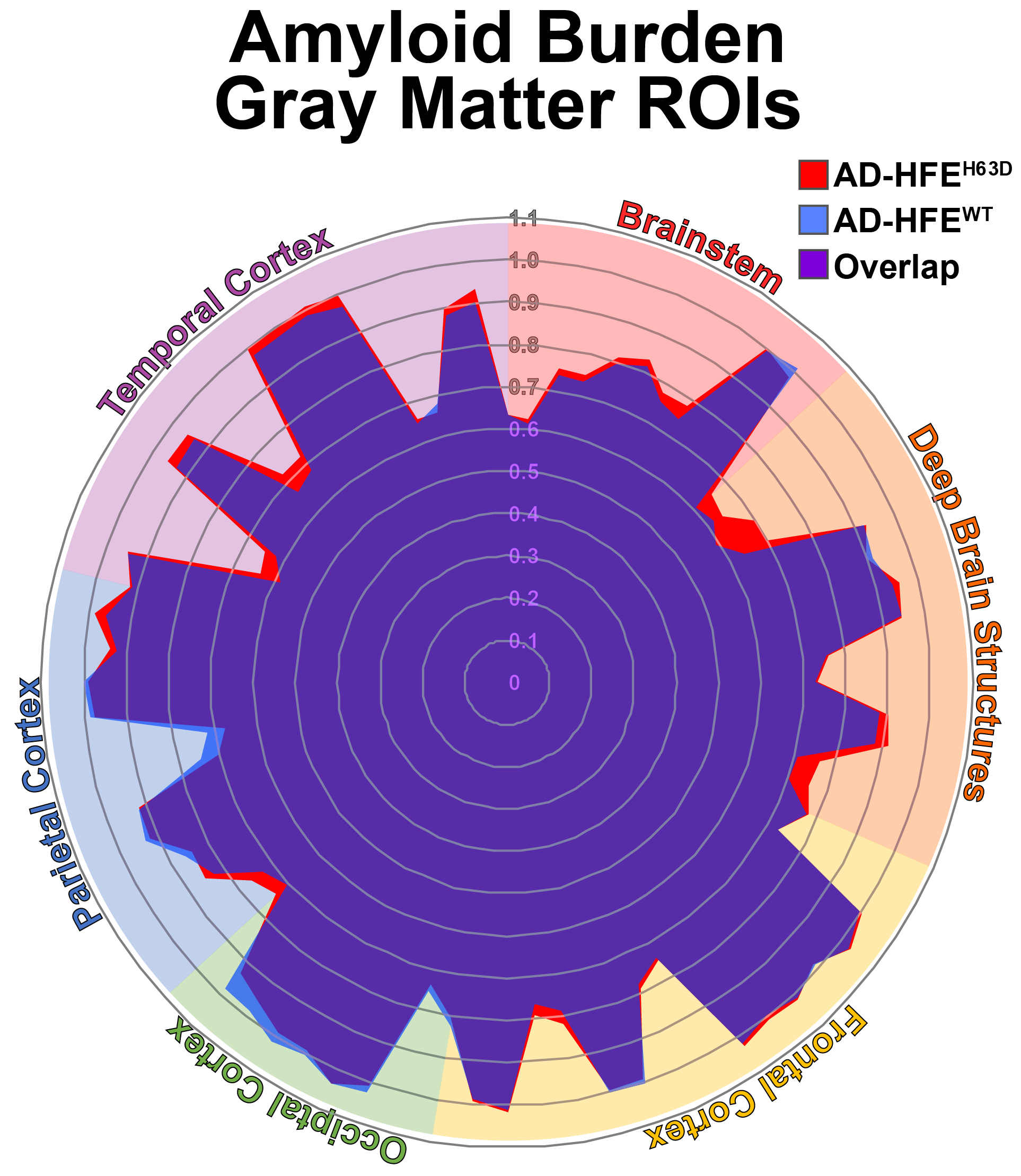
Figure
4 – AV-45 PET imaging of amyloid burden in AD HFE carriers. HFEH63D AD carriers have an
increase in cortical amyloid load in the temporal, parietal, and frontal
cortices.
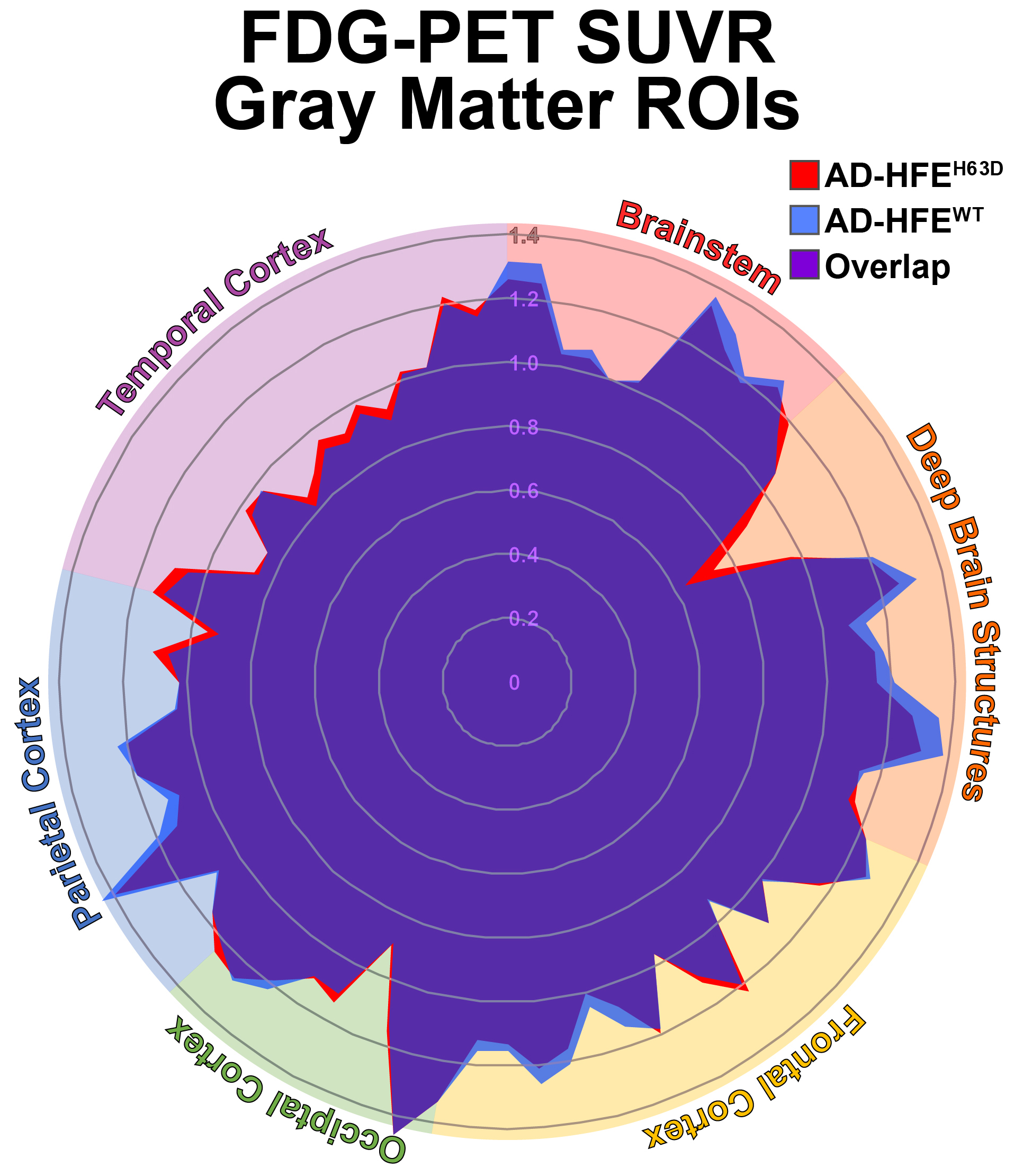
Figure
5 – FDG-PET imaging of glucose metabolism in AD HFE carriers. HFEH63D AD carriers have an increased
in metabolism in temporal structures and decrease in metabolism in parietal,
frontal, and deep brain structures.