3050
An extended-2D CNN approach for diagnosis of Alzheimer’s disease through structural MRI1Medical Image Computing Laboratory, School of Electrical and Computer Engineering, University of Campinas (UNICAMP), Campinas, Brazil
Synopsis
Alzheimer's disease (AD) is a devastating type of dementia that affects millions of people around the world. To date, there is no cure for Alzheimer's and its early-diagnosis has been a challenging task. The current techniques for AD diagnosis have explored the structural information of MRI. The aim of this work is to investigate the use of 2D-CNN approaches to distinguish AD patients from MCI and NC using T1-weighted MRI, since most of the works either explored the classic machine-learning or 3D-CNN approaches. The main novelty of our methodology is the use of an extended-2D approach, which explores the volumetric information of the MRI data while maintaining the low costs associated with a 2D approach.
INTRODUCTION
Alzheimer's disease (AD) is a devastating type of dementia that affects millions of people around the world1. To date, there is no cure for Alzheimer's and its early-diagnosis has been a challenging task. The current techniques for image-based AD diagnosis have explored the structural information of Magnetic-Resonance Imaging (MRI)2. Among these techniques, deep convolutional neural networks (CNN) is the most promising one and has been successfully used specially in medical images for a variety of applications due to its ability of features extraction. Before deep learning and CNNs, works that aimed to classify the different stages of AD, i.e. normal cohort (NC), mild-cognitive impairment (MCI), and the pathologically proven AD stage, explored classic machine-learning approaches and a meticulous feature engineering. After the success of deep learning in a variety of problems, works trying to predict the different AD stages began to explore this technique, most of them using 3D-CNN approaches.
The aim of this work is to investigate the use of 2D-CNN approaches to distinguish AD patients from MCI and NC using T1-weighted MRI, since most of the works either explored the classic machine-learning approaches, largely dependable of hand crafted features, or 3D-CNN costly approaches. The main novelty of our methodology is the use of an extended-2D approach, which explores the MRI volumetric data information while maintaining the low computational costs associated with a 2D approach, when compared to 3D-CNNs.
METHODS
The dataset is composed of 582 T1-weighted MRI volumes from Alzheimer's Disease Neuroimaging Initiative3 (ADNI) dataset, being distributed in 189 NC, 193 MCI, and 200 AD balanced by genre and age. Firstly, we pre-processed our data by rescaling it to isometric, skull-stripping using CONSNet4, brain registration using the FLIRT5 function on FSL, and intensity normalization. The slice selection of each 3D MRI volume was performed in two steps. Starting from the central slice, every other second slice was selected, until there were 20 slices on each side. These slices were used as the first channel of the CNN. Then, the remaining two channels were chosen by skipping 3 and 7 slices from the first channel, respectively. For example, if the position of a given slice of the first selection was 100, the position of the other two selected slices would be 104 and 108. By the end, from each 3D MRI, we selected 40 images being each image composed by three channels, where each channel corresponds to a different slice selected (Fig 1).
RESULTS AND DISCUSSION
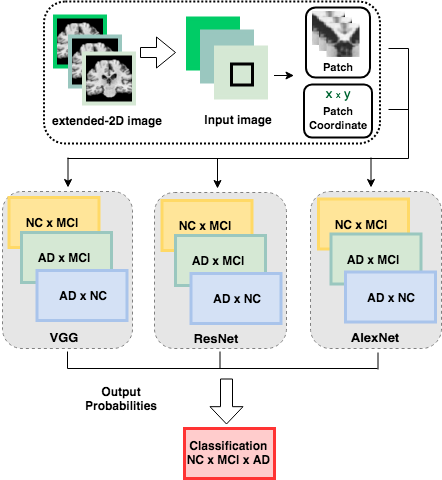
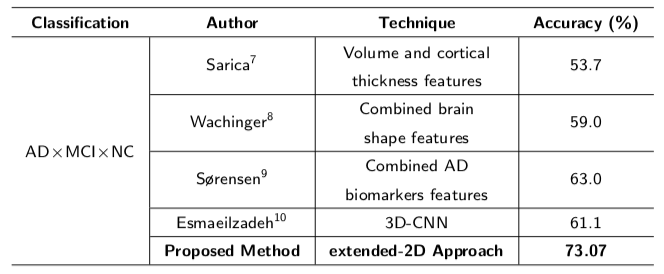
We trained an ensemble architecture presented in Fig 2 using 23,280 input images being 70% for training, 20% for validation, and 10% for test. Input images were generated using the RandomCrop data-augmentation function by randomly cropped 64x64 patches from each image. We also extracted the coordinates of each patch in the original image. Subsequently, we combined the resulting features derived from pre-trained CNN layers, with the corresponding patch coordinates in a full connected layer, following by the classification layer. The experiments were built and implemented based on the Pytorch4 implementation of the pre-trained CNN models and the performance was assessed by calculating the accuracy metric. To evaluate the model, a 2-fold cross-validation randomly split the dataset into sets of training (70%) and validation (20%). Besides, we investigated the effects of the main hyperparameters, and our best result had the following parameters: Cross-Entropy as our loss function, Adam as our optimizer with a learning-rate of 5×10-4, number of trained epochs was 1000. Table 1 gives the accuracy results computed by subject (not single images) of our model and a comparison of classification performance with other techniques. Our approach achieved an accuracy of 73.07%, considerably higher than the method proposed by Esmaeilzadeh10 (61.1%). It is interesting to point out that our proposal is the only 2D approach, while the others either explored traditional machine learning or 3D-CNN approaches. The proposed work not only has a better accuracy, but is also more computationally efficient when compared to 3D-CNN models. Another advantage is the possibility of using deeper networks, thus extracting more features. In addition, the proposed model does not require any feature engineering technique, which the classic machine learning models are more likely dependable to obtain good results.
CONCLUSION
In this work, we developed an extended-2D-CNN model to diagnose AD stages using MRI. Instead of formulating the AD diagnosis as binary classification only, we presented the diagnosis task taking into account the diseases progression and degeneration. Our approach not only led to the best classification performance compared to other methods but also contributed to our 2D data exploration. We compared the performance of our model with other methods and our result overcomes the other strategies for the 3-class classification.
Acknowledgements
We would like to thank the Brazilian National Council for Scientific and Technological Development (CNPq – process 308311/2016-7 and 168468/2017-4) and FAPESP (process CEPID 2013/07559-3).References
1. Dennis J Selkoe. Alzheimer’s disease: genes, proteins, and therapy. Physiological reviews, 81(2):741–766, 2001.
2. Litjens, Geert, et al. "A survey on deep learning in medical image analysis." Medical image analysis 42 (2017): 60-88.
3. Susanne G Mueller, Michael W Weiner, Leon J Thal, Ronald C Petersen, Clifford R Jack, William Jagust, John QTrojanowski, Arthur W Toga, and Laurel Beckett. Ways toward an early diagnosis in alzheimer’s disease: the alzheimer’sdisease neuroimaging initiative (adni).Alzheimer’s & Dementia, 1(1):55–66, 2005.
4. Oeslle Lucena, Roberto Souza, Leticia Rittner, Richard Frayne, and Roberto Lotufo. Convolutional neural networksfor skull-stripping in brain mr imaging using consensus-based silver standard masks.arXiv preprint arXiv:1804.04988,2018
5. Mark Jenkinson and Stephen Smith. A global optimisation method for robust affine registration of brain images.Medical image analysis, 5(2):143–156, 2001.
6. Adam Paszke, Sam Gross, Soumith Chintala, Gregory Chanan, Edward Yang, Zachary DeVito, Zeming Lin, AlbanDesmaison, Luca Antiga, and Adam Lerer. Automatic differentiation in pytorch. 2017.
7. Alessia Sarica, Giuseppe Di Fatta, G Smith, Mario Cannataro, James Douglas Saddy, et al. Advanced featureselection in multinominal dementia classification from structural mri data. InProc MICCAI Workshop Challenge onComputer-Aided Diagnosis of Dementia Based on Structural MRI Data, pages 82–91, 2014
8. C Wachinger, K Batmanghelich, P Golland, and M Reuter. Brainprint in the computer-aided diagnosis of alzheimer’sdisease.Challenge on Computer-Aided Diagnosis of Dementia, MICCAI, 2014.
9. Lauge Sørensen, Akshay Pai, Cecilie Anker, Ioana Balas, Martin Lillholm, Christian Igel, and Mads Nielsen. Dementiadiagnosis using mri cortical thickness, shape, texture, and volumetry. InProc MICCAI workshop challenge oncomputer-aided diagnosis of dementia based on structural MRI data, pages 111–118, 2014.
10. Esmaeilzadeh, Soheil, et al. "End-To-End Alzheimer’s Disease Diagnosis and Biomarker Identification." International Workshop on Machine Learning in Medical Imaging. Springer, Cham, 2018.
11. Esther E Bron, Marion Smits, Wiesje M Van Der Flier, Hugo Vrenken, Frederik Barkhof, Philip Scheltens, Janne MPapma, Rebecca ME Steketee, Carolina Mendez Orellana, Rozanna Meijboom, et al. Standardized evaluation of al-gorithms for computer-aided diagnosis of dementia based on structural mri: the caddementia challenge.NeuroImage,111:562–579, 2015.
Figures
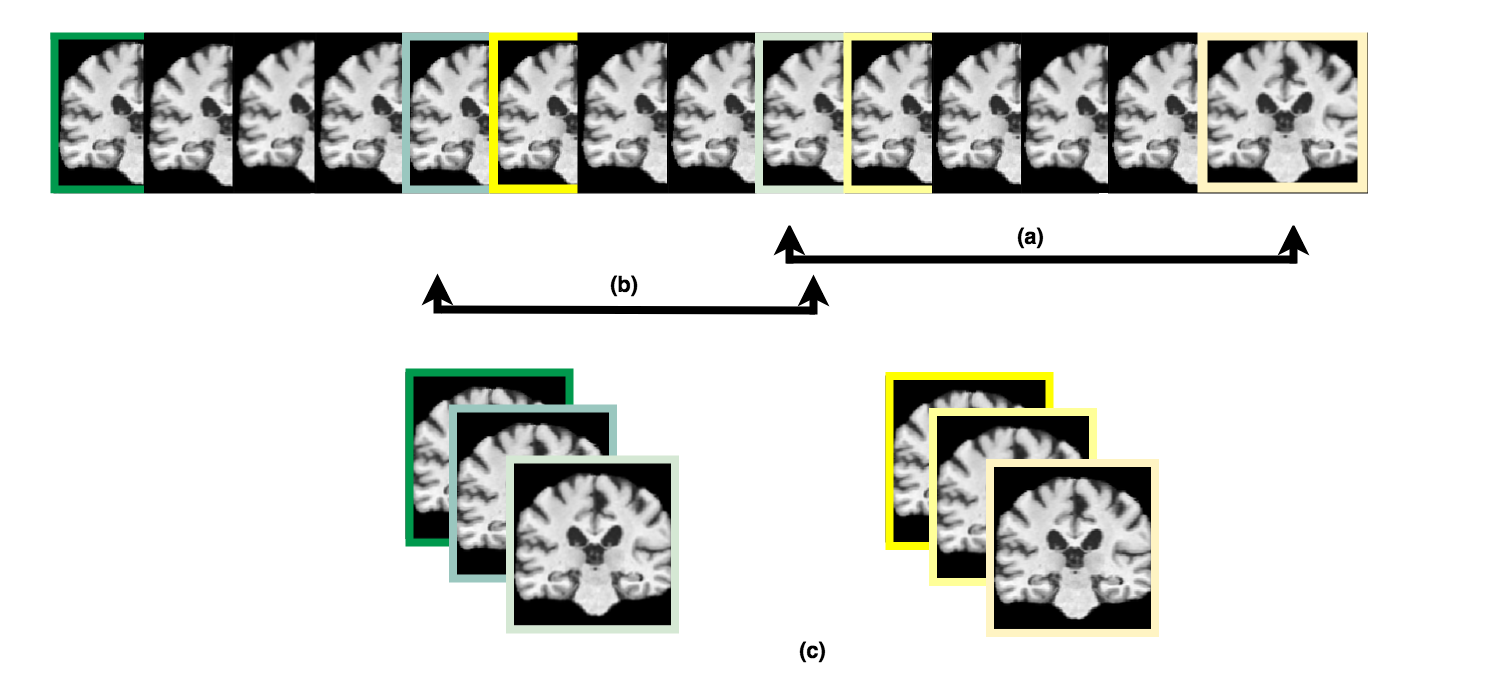
Figure 1: Slices selection of each 3D MRI: (a) starting from the central slice, every other second slice was selected, until there were 20 slices on each side. These slices were used as the first channel of the CNN, (b) then, the remaining two channels were chosen by skipping 3 and 7 slices from the first channel, respectively. By the end, from each 3D MRI, we selected 40 images being each image composed by three channels, where each channel corresponds to a different slice selected, (c) the final extended-2D input images.