3041
MRI study of cortical thickness and regional brain volume in pediatric cancer survivorsPatricia Stefancin1, Christine Cahaney1, Robert Parker2, Thomas Preston1, Jessica Goldstein1, Rina Meyer2, Cara Giannillo1, Debra Giugliano1, Tim Duong1, and Laura Hogan2
1Stony Brook Medicine, Stony Brook, NY, United States, 2Stony Brook Children's Hospital, Stony Brook, NY, United States
Synopsis
The concept of pediatric chemobrain and the neural mechanisms that underlie its development have not been adequately studied. In this study, MRI was used to examine the neuroanatomy of childhood cancer survivors. We found reduced brain volumes and cortical thicknesses in childhood cancer survivors compared to age-matched controls. These changes were in regions known to be involved in working-memory function and executive function, which could account for the development of executive function difficulties observed in childhood cancer survivors. These findings may prove useful to inform treatment strategies and modify behavioral programs to help survivors combat these issues.
Introduction
Improved cancer treatments have resulted in longer survival of childhood cancer patients 1, 2. However, many survivors show difficulties in working memory, attention, cognitive switching, and visuospatial distortion, which have been attributed to chemotherapies used3-5 (ca. chemobrain). Although chemobrain has been well studied in breast cancer survivors, it has not been adequately studied in pediatric cancer patients. This study tested the hypothesis that chemotherapy-treated pediatric cancer survivors show reduced regional brain volumes and cortical thickness when compared to age-matched controls.Methods
Fifteen chemotherapy-treated childhood cancer survivors diagnosed with a non-central nervous system cancer before the age of 18 and seventeen healthy age-matched controls were studied. Exclusions included prior cranial radiation therapy, known neuropsychiatric disorders, or contraindications for MRI. To evaluate for memory, attention and fine motor skills, subjects underwent the NEPSY-II, Purdue Pegboard and N-back working-memory tasks (0-back and 2-back paradigm). Parents also completed the Behavioral Rating Inventory of Executive Functioning (BRIEF) Parental Rating. Subjects completed a 3D-MPRAGE MRI at 3T (TR=2300ms, TE=3.24ms, FOV=223x223 mm, thk=0.87mm, and 0.9x0.9x0.9mm). Structural volumes were normalized to MNI space, and segmented using tissue probability maps. Voxel-based morphometry (VBM) and cortical thickness analysis were performed using CAT12 toolbox for SPM. Subcortical volumetric analysis was performed using FSL FIRST. Statistical and correlation analysis were performed using SPSS.Results
Compared to controls, patients showed smaller total-brain volume (T=-2.1, p=0.043), gray-matter (T=-2.2, p=0.03), and white-matter (T=-2.1, p=0.046) volumes. VBM analysis showed smaller gray-matter volume in patients in the right orbitofrontal area (T=-5.1, p=0.001), right anterior prefrontal cortex (T=-4.8, p=0.001), and right supramarginal gyrus (T=-4.5, p=0.030) compared to controls. Cortical thickness analysis showed thinning of the right temporal pole (T=-6.2, p=0.002) and thickening of the right parahippocampal gyrus in the patient group. Patients revealed reduced volume in the right thalamus (T=-4.01, p=0.001), left thalamus (T=-4.6, p<0.001), and left nucleus accumbens (T=-3.2, p=0.004). On the working-memory task, patients had fewer correct responses and more incorrect and no-responses than controls. They also had longer response times on all trials compared to controls. The number of correct answers positively correlated with total brain volume (R2=0.459, p=0.018) and white-matter volume (R2=0.453, p=0.023) while the number of incorrect negatively correlated with total brain volume (R2=-0.424, p=0.031) and white-matter volume (R2=0.424, p=0.031). The number of no-response trials negatively correlated with the right thalamus volume (R2=-0.366, p=0.006) and the left nucleus accumbens volume (R2=-0.730, p<0.001). Patients showed deficits by NEPSY-II and Purdue Pegboard scores but none by BRIEF total score or sub-scores compared to normative data. However, these results did not significantly correlate with differences in regional brain volumes or cortical thicknesses.Discussion
The anterior prefrontal cortex and supramarginal gyrus are involved in working memory function, albeit distinct components, as demonstrated by individuals with damage to these areas 7,8,9. The orbitofrontal area is associated with higher order reasoning and decision making8 while the thalamus is one of the major relay stations in the brain. These areas are involved in working memory, decision-making, and the relaying and processing of information. It is conceivable that they play some role in poorer working memory performance given the correlations observed between decreased global brain and white matter volumes with inferior performance on the working memory task. The right temporal pole also showed reduced cortical thickness which may be significant given that it is involved in memory retrieval, something known to be deficient in childhood cancer survivors 10. Alternatively, the cortical thickening of the right parahippocampal gyrus, which is known to be involved in memory encoding and retrieval, was increased in patients. Although it may seem contradictory, this cortical thickening may be associated with increased effort in memory and coordination tasks reported by chemobrain patients. There are only a handful of other studies on volumetric changes in pediatric cancer survivors. Neurocognitive scores measuring working memory and inhibition were correlated with the volumes of the amygdala, 11. No papers documented changes in cortical thickness.Conclusion
Chemotherapy in pediatric cancer survivors likely caused changes in regional brain volumes and cortical thickness consistent with problems that survivors face with working memory and cognitive function.Acknowledgements
No acknowledgement found.References
. Kaiser J, Bledowski C, Dietrich J. Neural correlates of chemotherapy-related cognitive impairment. Cortex. 2014;54:33-50. 2. Campbell LK, Scaduto M, Sharp W, et al. A meta-analysis of the neurocognitive sequelae of treatment for childhood acute lymphocytic leukemia. Pediatr Blood Cancer. 2007;49(1):65-73. 3. Anderson FS, Kunin-Batson AS. Neurocognitive late effects of chemotherapy in children: the past 10 years of research on brain structure and function. Pediatr Blood Cancer. 2009;52(2):159-164. 4. Robinson KE, Livesay KL, Campbell LK, et al. Working memory in survivors of childhood acute lymphocytic leukemia: functional neuroimaging analyses. Pediatr Blood Cancer. 2010;54(4):585-590. 5. Jacola LM, Krull KR, Pui CH, et al. Longitudinal Assessment of Neurocognitive Outcomes in Survivors of Childhood Acute Lymphoblastic Leukemia Treated on a Contemporary Chemotherapy Protocol. J Clin Oncol. 2016;34(11):1239-1247. 6. Jim HS, Phillips KM, Chait S, et al. Meta-analysis of cognitive functioning in breast cancer survivors previously treated with standard-dose chemotherapy. J Clin Oncol. 2012;30(29):3578-3587. 7. Ramnani N, Owen AM. Anterior prefrontal cortex: insights into function from anatomy and neuroimaging. Nat Rev Neurosci. 2004;5(3):184-194. 8. Rudebeck PH, Rich EL. Orbitofrontal cortex. Curr Biol. 2018;28(18):R1083-R1088. 9. Russ MO, Mack W, Grama CR, et al. Enactment effect in memory: evidence concerning the function of the supramarginal gyrus. Exp Brain Res. 2003;149(4):497-504. 10. Chadwick MJ, Anjum RS, Kumaran D, et al. Semantic representations in the temporal pole predict false memories. Proc Natl Acad Sci U S A. 2016;113(36):10180-10185. 11. Aminoff EM, Kveraga K, Bar M. The role of the parahippocampal cortex in cognition. Trends Cogn Sci. 2013;17(8):379-390.Figures
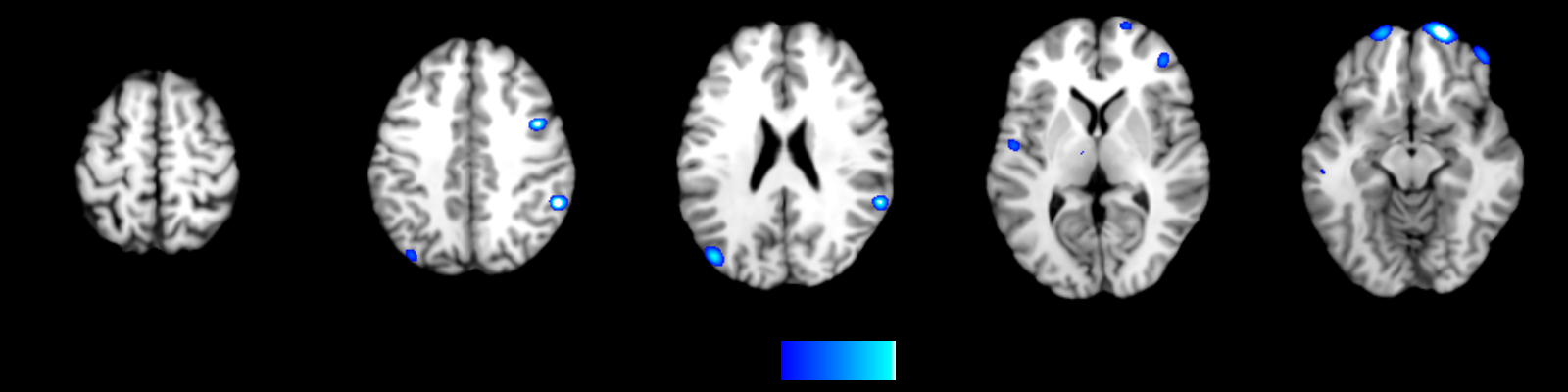
VBM analysis results
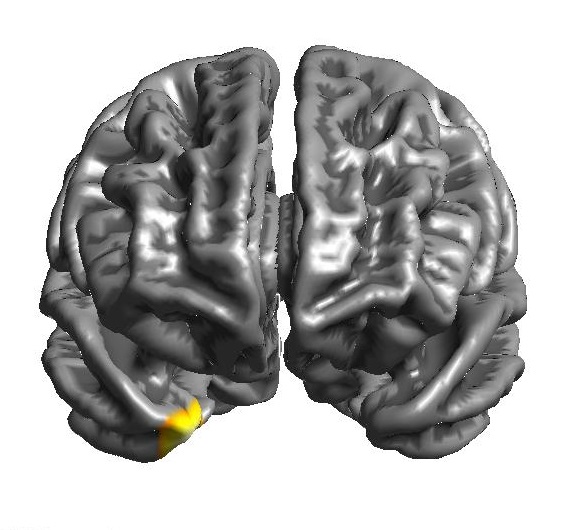
Cortical thickness results: Temporal Pole
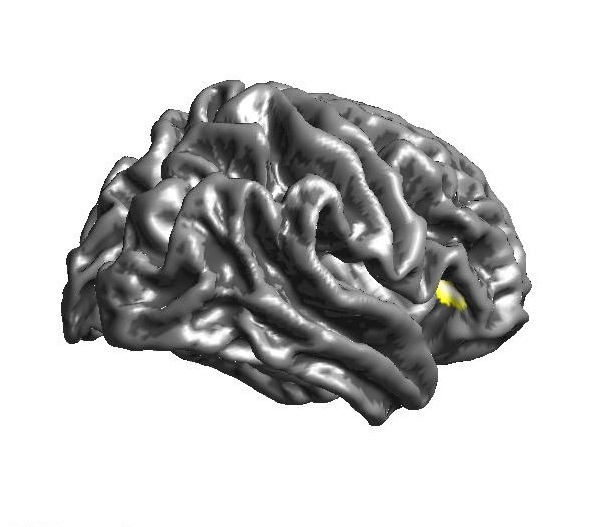
Cortical thickness results: Parahippocampal gyrus