3038
Quantifying changes in excitation and inhibition in childhood migraine1Department of Radiology, University of Calgary, Calgary, AB, Canada, 2Hotchkiss Brain Institute, University of Calgary, Calgary, AB, Canada, 3Alberta Children's Hospital Research Institute, University of Calgary, Calgary, AB, Canada, 4Department of Psychology, University of Calgary, Calgary, AB, Canada, 5Department of Clinical Neurosciences, University of Calgary, Calgary, AB, Canada, 6Hotchkiss Brain Institute, Alberta Children's Hospital Research Institute, Calgary, AB, Canada
Synopsis
Though migraine is one of the top five most common childhood diseases, there has been relatively little investigation into migraine in children. There is evidence of abnormal excitability in the cortex of children with migraine, but levels of excitatory and inhibitory neurotransmitters have not been investigated. We used MRS to compare levels of the neurotransmitters GABA (inhibitory) and Glx (glutamate + glutamine; excitatory) between children with migraine and typically developing controls. We found no significant difference in neurotransmitter levels in the brain of children with migraine; however we found a relationship between neurotransmitter levels and migraine characteristics.
Introduction
Migraine is a neurological disorder, characterised by recurrent, often severe and debilitating headache attacks, and other associated neurological symptoms. Migraine is one of the top five most common childhood diseases, affecting over 10% of children aged 5-151.Early intervention can decrease migraine frequency, with those receiving earlier interventions more likely to achieve remission. However, treatment strategies for children are limited, in part due to limited knowledge about pediatric migraine biology, and the main medications used to treat or prevent migraine in adults are often ineffective in children2.
There is increasing evidence that adult migraine results from an imbalance of excitation/inhibition in the brain. Specifically, neurophysiological studies suggest the cortex is hyper-excited as a result of abnormal thalamic control3. In adults with migraine, GABA (primary inhibitory neurotransmitter) and glutamate (primary excitatory neurotransmitter) levels have been shown to differ relative to controls in multiple brain areas4. For example, adults with migraine show increased glutamate5 and decreased GABA6 in the visual cortex.
Despite evidence of abnormal excitability of the sensory cortex in children with migraine, as demonstrated by increased brain activation observed using magnoelectroencephalogrophy7, GABA and glutamate levels remain uninvestigated. Understanding this neurochemistry is essential to develop effective interventions for pediatric migraine.
Method
Nine children with migraine (3 female, 7-11yrs, Mage=9.6yrs) and 14 age-matched typically developing children (7 female, Mage=9.5y) were recruited. Children with migraine completed a migraine diary for one month prior to and 7 days after being scanned. This daily report indicates whether they had a headache, pain intensity and length.
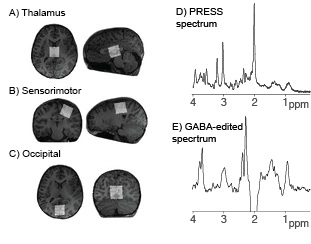
Scanning was performed on a 3T GE 750w MR scanner using a 32-channel head coil. A whole-brain T1-weighted structural image was acquired for voxel placement and tissue segmentation. 3x3x3cm3 voxels were placed in the thalamus (midline centred), right sensorimotor cortex and the occipital cortex (midline centred; Figure 1). MEGA-PRESS (TR/TE = 1800/80ms, 20ms editing pulses alternating between 1.9 ppm and 1.5 ppm; 256 averages) was used to acquire macromolecule-suppressed GABA data. MEGA-PRESS data were analysed using Gannet3.08, including tissue correction9. A short-echo PRESS sequence (TR/TE = 1800/35ms; 64 averages) was used to measure glutamate (quantified as the combined signals of glutamate and glutamine, Glx). PRESS data were analysed using LCModel10, and metabolite values were corrected for tissue composition11. Data quality was assessed by visual inspection and metabolite linewidth, spectra with a linewidth over 0.1 ppm were excluded.
Results
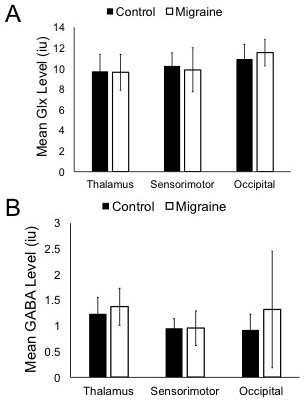
GABA and Glx levels were not significantly different between children with migraine and typically developing controls in any of the three voxels (Figure 2).
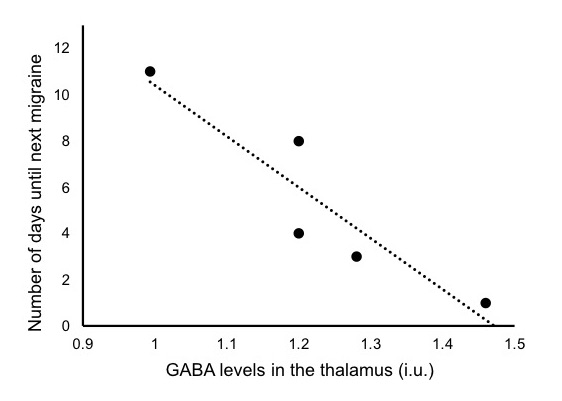
There was a significant negative correlation between GABA in the thalamus and the number of days until the next migraine occurred (r=-0.918, p = 0.028, n=5; Figure 3). Those with higher GABA in the thalamus experienced a migraine sooner.
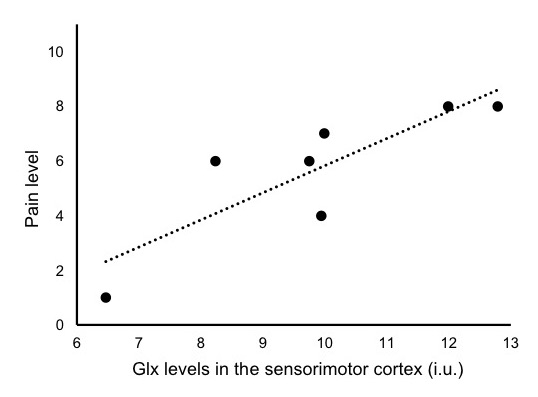
There was a significant positive correlation between Glx in the sensorimotor cortex and the pain level of the previous migraine (r=0.847, p = 0.016, n=7; Figure 4). Those with higher Glx levels in the sensory motor cortex reported higher pain intensity during the preceding migraine (mean days previously = 3.5, SD = 2.76).
Discussion and Conclusion
Previous studies in adult migraine have shown altered levels of the neurotransmitters GABA and Glx in various brain regions4. Our results show no significant differences in GABA or Glx in children with migraine compared to typically developing controls. As pediatric migraine presentation is different from adults, this finding may not be surprising. Indeed, topiramate, a glutamate receptor antagonist which results in increased GABA, is commonly used to prevent adult migraine but has no effect in children12. This emphasizes the need to further investigate migraine neurobiology in children, rather than extrapolating from adult studies.
Adult research has shown correlations between inhibition in the somatosensory cortex and migraine characteristics of pain and frequency. Furthermore lateral inhibition and its alterations in the somatosensory cortex has been correlated with thalamocortical activation changes3. Our results showing correlations between (a) thalamic GABA and the time until the next migraine and (b) somatosensory glutamate and pain intensity of the previous migraine are consistent with alterations in cortical excitation and inhibition dynamics in migraine. Moreover, these results support the notion that these alterations in excitation and inhibition are dependent on the phase of the migraine cycle.
While these results are preliminary, to our knowledge, this is the first time that associations in GABA and glutamate have been shown with migraine characteristics in pre-pubertal migraine. These results emphasize the need to further investigate migraine in children to describe the underlying biology to assist in developing earlier, improved diagnoses and identify potential targets for intervention.
Acknowledgements
This study was funded by the SickKids Foundation and the Canadian Institute for Health Research (CIHR-IHDCYH)References
1. Maleki N, Bernstein C, Napadow V, Field A. Migraine and Puberty: Potential Susceptible Brain Sites. Semin. Pediatr. Neurol. 2016;23:53–59 doi: 10.1016/j.spen.2016.01.011.
2. Kroon Van Diest AM, Ernst MM, Slater S, Powers SW. Similarities and Differences Between Migraine in Children and Adults: Presentation, Disability, and Response to Treatment. Curr. Pain Headache Rep. 2017;21 doi: 10.1007/s11916-017-0648-2.
3. Coppola G, Bracaglia M, Di Lenola D, et al. Lateral inhibition in the somatosensory cortex during and between migraine without aura attacks: Correlations with thalamocortical activity and clinical features. Cephalalgia 2015;36:568–578 doi: 10.1177/0333102415610873.
4. Younis S, Hougaard A, Vestergaard MB, Larsson HBW, Ashina M. Migraine and magnetic resonance spectroscopy: A systematic review. Curr. Opin. Neurol. 2017;30:246–262 doi: 10.1097/WCO.0000000000000436.5. González De La Aleja J, Ramos A, Mato-Abad V, et al. Higher glutamate to glutamine ratios in occipital regions in women with migraine during the interictal state. Headache 2013;53:365–375 doi: 10.1111/head.12030.
6. Bridge H, Stagg CJ, Near J, Lau CI, Zisner A, Zameel Cader M. Altered neurochemical coupling in the occipital cortex in migraine with visual aura. Cephalalgia 2015;35:1025–1030 doi: 10.1177/0333102414566860.
7. Leiken KA, Xiang J, Curry E, et al. Quantitative neuromagnetic signatures of aberrant cortical excitability in pediatric chronic migraine. J. Headache Pain 2016;17 doi: 10.1186/s10194-016-0641-x.
8. Edden RAE, Puts NAJ, Harris AD, Barker PB, Evans CJ. Gannet: A Batch-Processing Tool for the Quantitative Analysis of Gamma-Aminobutyric Acid–Edited MR Spectroscopy Spectra. J Magn Reson Imaging 2014;40:1445–1452 doi: 10.1038/jid.2014.371.
9. Harris AD, Puts NAJ, Edden RAE. Tissue correction for GABA-edited MRS: Considerations of voxel composition, tissue segmentation, and tissue relaxations. J. Magn. Reson. Imaging 2015;42:1431–1440 doi: 10.1002/jmri.24903.
10. Provencher SW. Automatic quantitation of localized in vivo 1H spectra with LCModel. NMR Biomed 2001;14:260–264.
11. Gasparovic C, Song T, Devier D, et al. Use of tissue water as a concentration reference for proton spectroscopic imaging. Magn. Reson. Med. 2006;55:1219–26 doi: 10.1002/mrm.20901.
12. Powers SW, Coffey CS, Chamberlin LA, et al. Trial of Amitriptyline, Topiramate, and Placebo for Pediatric Migraine. N. Engl. J. Med. 2017;376:115–124 doi: 10.1056/NEJMoa1610384.
Figures