3024
INCORPORATING MRS BIOMARKERS INTO MULTICENTER CLINICAL TRIALS: QUALITY ASSURANCE RESULTS FROM THE HIGH-DOSE ERYTHROPOIETIN FOR ASPHYXIA AND ENCEPHALOPATHY (HEAL) TRIAL1Radiology, Children's Hospital Los Angeles, Los Angeles, CA, United States, 2Fetal and Neonatal Institute, Division of Neonatology, CHLA Dept. of Pediatrics, University of Southern California, Los Angeles, CA, United States, 3Neurology, University of California, San Francisco, San Francisco, CA, United States, 4Radiology, University of Pittsburgh, Pittsburgh, PA, United States, 5Pediatrics, Division of Neonatology, Washington University, St. Louis, MO, United States, 6Pediatrics, Division of Neonatology, University of Washington, Seattle, WA, United States, 7Radiology, Washington University, St. Louis, MO, United States
Synopsis
MR Spectroscopy (MRS) provides early biomarkers of brain injury and treatment response in neonates with hypoxic-ischemic encephalopathy. We present preliminary data from the High-dose Erythropoietin for Asphyxia and Encephalopathy (HEAL) Trial (NCT02811263), comparing quality assurance parameters across MR vendors. Overall, we have been able to analyze MRS data obtained from 85% of patients who underwent MRI, although this rate is lower at sites operating GE MR systems. 92% of spectra met quality standards, with slight differences in FWHM and SNR by vendor. Overall, these data demonstrate the feasibility of obtaining reliable MRS data in a multicenter neonatal randomized controlled trial.
INTRODUCTION
MR Spectroscopy (MRS) provides early biomarkers of brain injury and treatment response in neonates with hypoxic-ischemic encephalopathy (HIE). However, in order for MRS biomarkers to be used as surrogate endpoints in multicenter clinical trials, it is necessary to establish that MRS data can be collected reliably across a diverse array of MR vendors and platforms. Here, we present quality assurance data from the High-dose Erythropoietin for Asphyxia and Encephalopathy (HEAL) Trial (NCT02811263)1. Our aim is to determine whether quality assurance parameters differ across MR vendors (Siemens, GE, Philips).
METHODS
HEAL is being carried out across a network of 17 study sites, including 5 with more than one enrolling hospital. The majority of sites are operating a Siemens 3T MR system (n=12), while the remainder operate a GE 3T (n=4), Philips 3T (n=4) or GE 1.5T MR system (n=2). All MRS data are obtained using a single-voxel point-resolved spectroscopy sequence using a standardized protocol, which includes a short-echo (TE 35 ms) and long-echo (TE 288 ms) spectra localized to the thalamus/posterior putamen and a short-echo (TE 35 ms) spectra localized to the parietal white matter. Aside from TE, all other parameters are held constant across 3T platforms (e.g., TR 2000, 128 signal averages). Following acquisition, MRS data are directly exported from the MR scanner, anonymized and uploaded to the HEAL Neuroimaging Core where they are reviewed for protocol compliance. MRS processing is carried out centrally using a standardized LCModel pipeline2. For this study, we compared protocol compliance parameters (e.g., MRS successfully acquired, MRS data uploaded) as well standard quality metrics calculated by LCModel (e.g., full-width half-maximum [FWHM], signal-to-noise [SNR]). Results were compared across vendors (Siemens, GE, Philips) using χ2 or ANOVA as appropriate.RESULTS
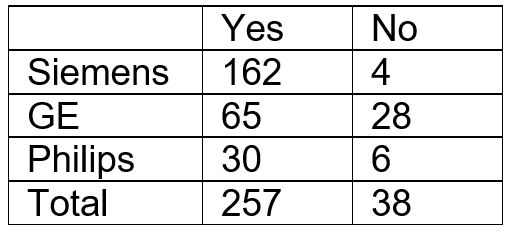
Of the first 320 patients enrolled, 301 underwent MRI and 295 underwent MRI + MRS. The reasons for missing MRI/S data include patient factors (e.g., uncooperative, parent refusal, early death) as well as technical factors (e.g., scanner being down). Of the 295 for whom MRS was acquired, 257 had raw data uploaded to the neuroimaging core. As shown in Table 1, the rate of successful data transfer was significantly lower for GE as compared to Siemens and Philips.
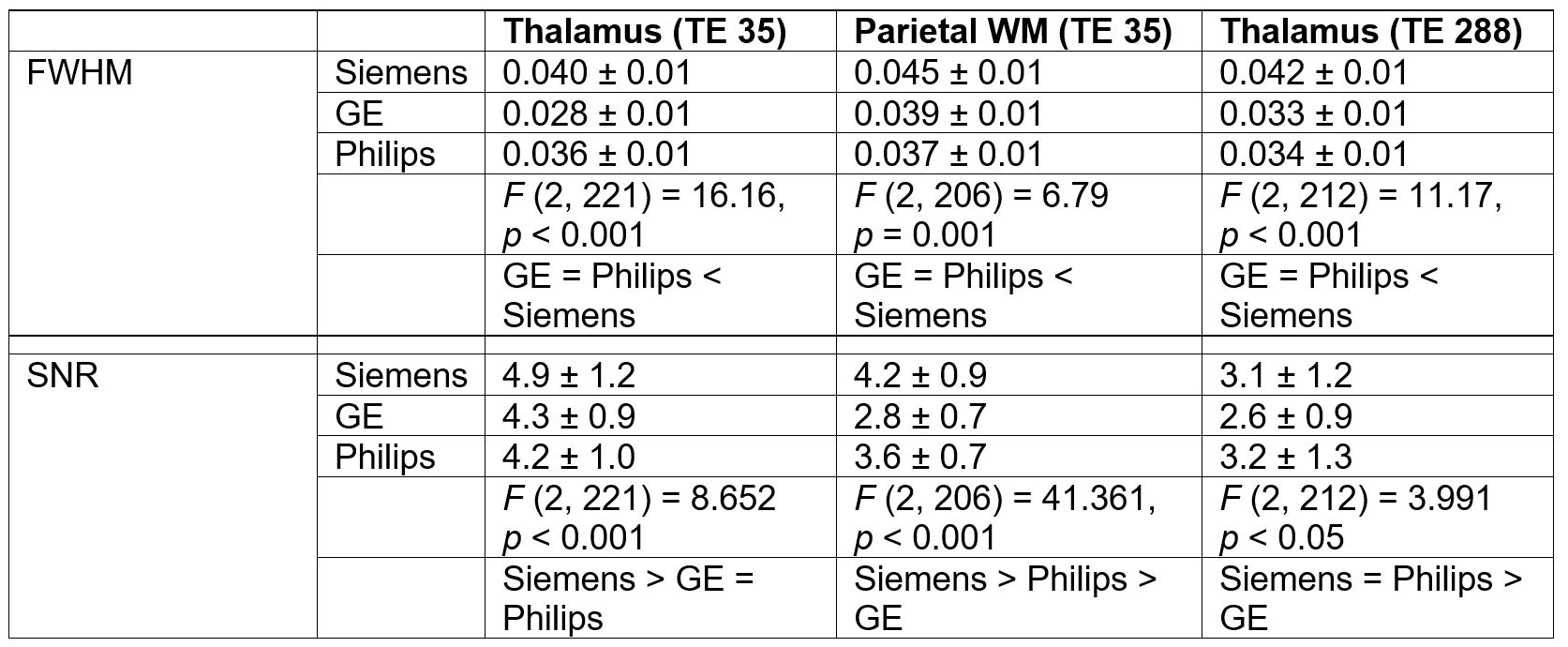
734 spectra obtained from the 257 patients were analyzed for quality, using a priori thresholds for FWHM and SNR. 61 (8%) of the acquired spectra did not meet quality standards. There were no differences by vendor (p > 0.1). Of 648 3T spectra that met quality thresholds, we compared FWHM and SNR across vendors for each of the three acquisitions. As shown in Table 2, linewidth (FWHM) was slightly worse on Siemens as compared to GE and Philips. However, SNR was slightly better on Siemens.
CONCLUSIONS
We obtained quantitative MRS data from 80% of the patients enrolled to date in the HEAL Trial and 85% of those who underwent MR imaging. Furthermore, 92% of the raw data met quality standards. To our knowledge, this is the largest RCT for neuroprotection to incorporate quantitative MRS biomarkers and the findings support that it is feasible to incorporate MRS biomarkers into multicenter clinical trials. To date, the biggest challenge in HEAL has been downloading and archiving the raw MRS data, which has been particularly problematic on GE scanners. This is not surprising considering that GE continues to use the P-file format, which is difficult to capture from the scanner in routine clinical workflow. By contrast, Siemens and Philips both permit direct export of raw MRS in dicom format, though not in a dicom format that permits archiving in standard PACS systems. In general, many of the challenges associated with incorporating MRS into multicenter clinical trials would be overcome if each vendor were to automatically archive raw MRS data in standard dicom format made compatible with PACS systems. Last, although we observed slight differences in both FWHM and SNR of spectra acquired on Siemens, GE and Philips MR Systems, it should be noted that the values above are all well within established parameters for quantitation.Acknowledgements
This study was carried out by the HEAL Study Group and would not have been possible without support from Radiology at each of the participating sites. The HEAL Trial is funded by the NIH (U01 NS092764, U01 NS092553).References
1 Juul SE, Comstock BA, Heagerty PJ, et al. High-Dose Erythropoietin for Asphyxia and Encephalopathy (HEAL): A Randomized Controlled Trial – Background, Aims, and Study Protocol. Neonatology 2018;98195:331–8. https://doi.org/10.1159/000486820.
2 Provencher SW. Automatic quantitation of localized in vivo1H spectra with LCModel. NMR Biomed 2001;14:260–4.
Figures