3021
Strategically Acquired Gradient Echo (STAGE) Imaging as a Means for Multi-Contrast Quantitative Pediatric Neuroimaging with Minimized Sedation: A Pilot Study in Sturge-Weber Syndrome1Department of Radiology, Wayne State University, Detroit, MI, United States, 2The MRI Institute for Biomedical Research, Bingham Farms, MI, United States, 3Department of Pediatrics, Wayne State University, Detroit, MI, United States
Synopsis
Non-sedated, non-contrast rapid pediatric magnetic resonance imaging methods are of great interest to pediatric radiology. In this work, we explore the possibility of a multi-contrast, quantitative method referred to as STAGE imaging for minimizing or eliminating sedation in Sturge-Weber Syndrome by using a k-space sharing strategy which increases the resolution of susceptibility weighted imaging and quantitative susceptibility mapping. Preliminary results show the potential of STAGE which generates more than 10 pieces of qualitative and quantitative information in one 5-minute protocol at 3T.
Introduction
MRI plays a significant role in pediatric neuroimaging but usually requires sedation or anesthesia. Sedation may cause long-term cognitive side effects and increases morbidity for children (1,2). To date, non-sedated methods or methods with minimal sedation are not well-studied but of great interest to pediatric radiologists. One practical way to reduce the need for sedation is to reduce scan time by only performing specific sequences for a certain clinical question and/or using a very low resolution, such as using a single shot fast spin echo (SSFSE) or half Fourier single shot turbo spin echo (HASTE) for quick T2 weighted imaging (3–5). However, there is always a need of multi-contrast images and quantitative data. Specifically, in patients with Sturge-Weber Syndrome (SWS), high-resolution susceptibility weighted imaging (SWI) and quantitative susceptibility mapping (QSM) are significant tools for studying calcification, impaired cortical veins and abnormal deep venous collaterals that commonly occur in SWS (6). In this study, we explore the possibility of a multi-contrast, quantitative method referred to as strategically acquired gradient echo (STAGE) imaging (7,8) for minimizing sedation in SWS and pediatric MRI. Furthermore, we propose a k-space sharing strategy to provide high-resolution SWI and QSM but maintaining the 5-minute scan time by acquiring the high frequency and low frequency parts in two consecutive RF pulse territories from different echoes.Methods
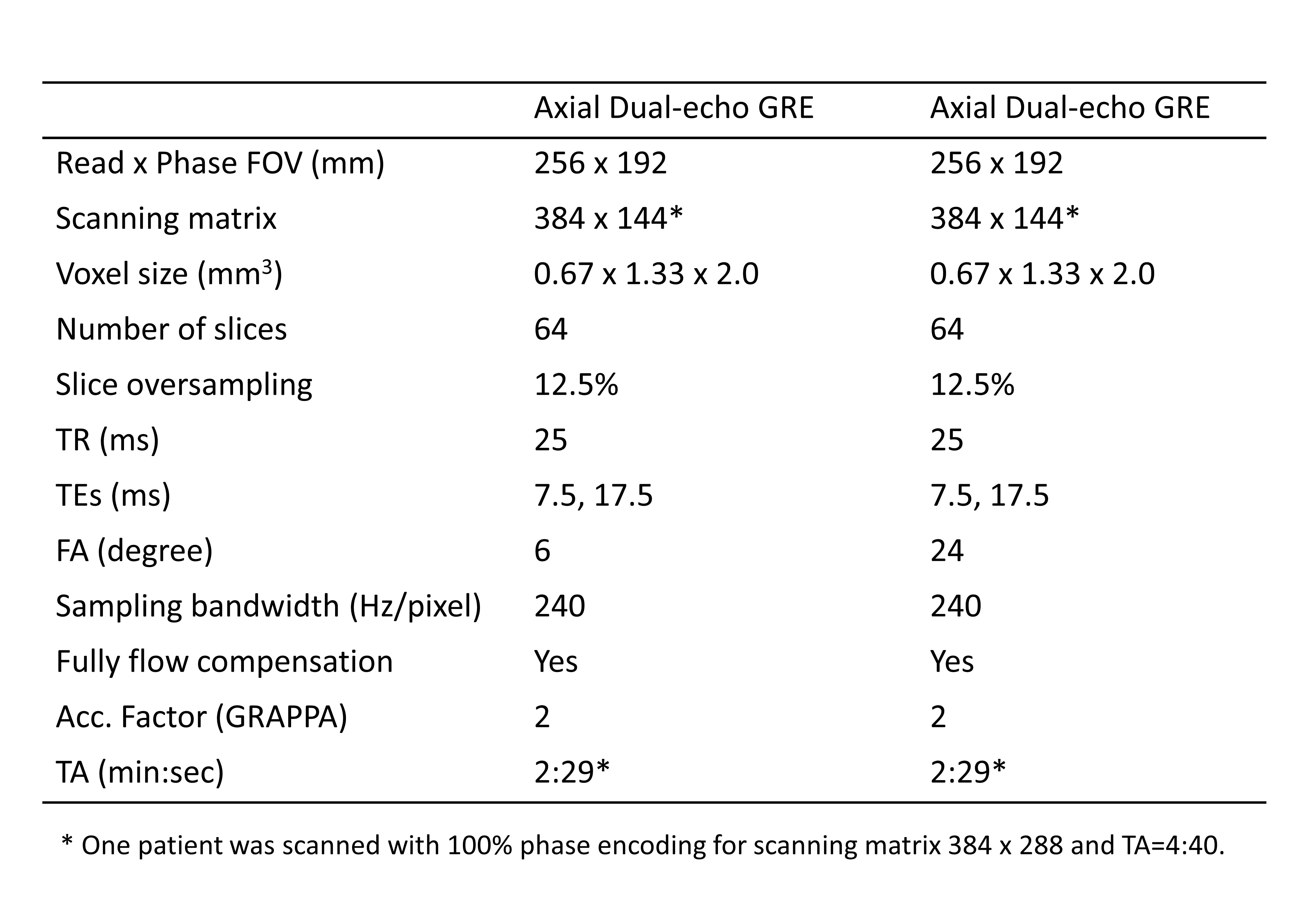
Data acquisition: Five patients with SWS (2 females and 3 males, average age 6-years and 8-months) were scanned, and this study was approved by the local IRB for imaging at 3T (Siemens Verio, Erlangen, Germany) using a 32-channel head coil. All children were sedated using an intravascular injection of 3mg/kg nembutal followed by 1μg/kg fentanyl prior to MRI scanning and monitored by a pediatric nurse who was well trained for sedation of children for radiological procedures. Two dual-echo GRE sequences were performed in 5 minutes with the parameters listed in Table-1. To obtain fully sampled high-resolution data for retrospectively evaluating the proposed k-space sharing strategy, one patient was scanned with 100% phase encoding, leading to a total of 9.3-minute scanning time for the two sequences.
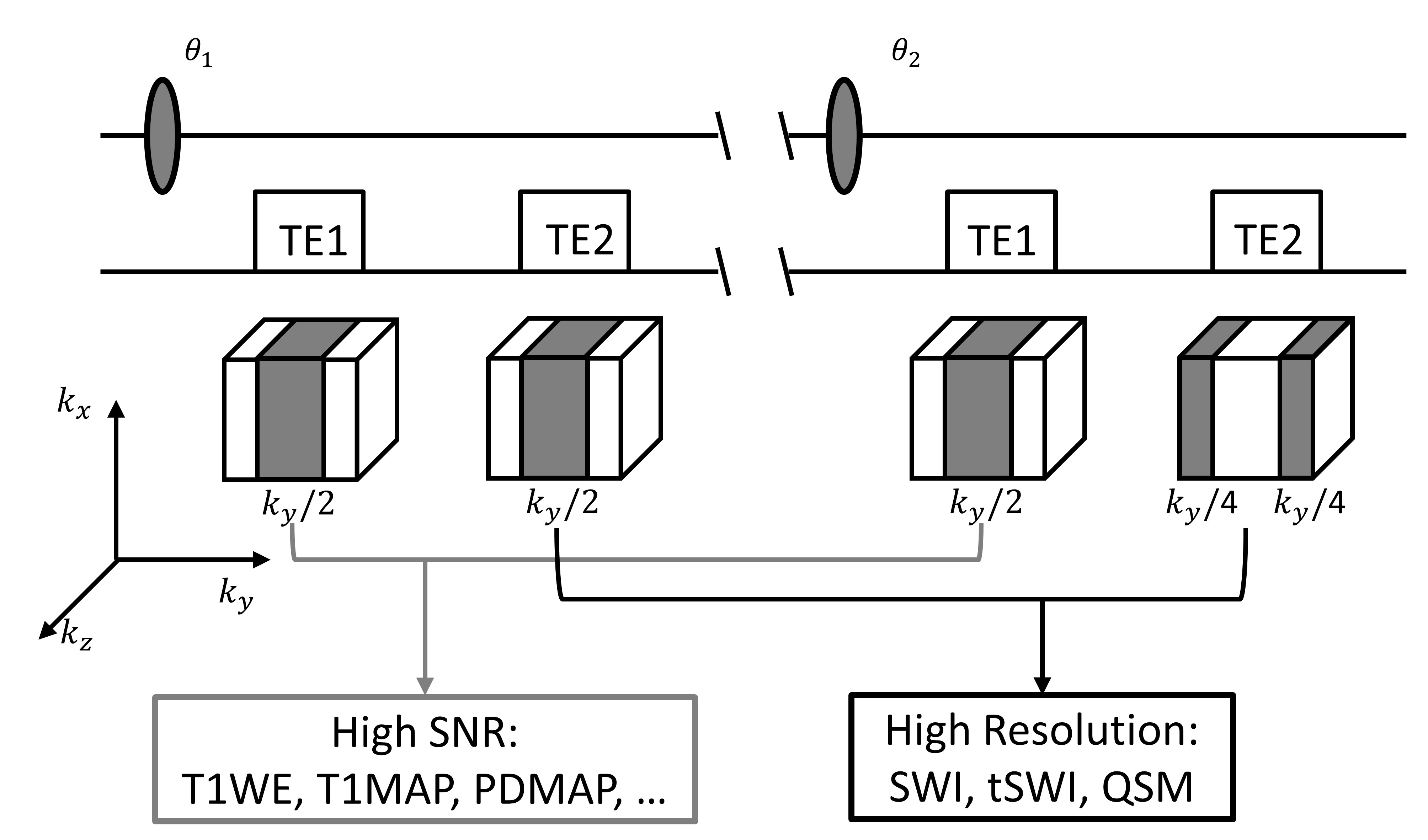
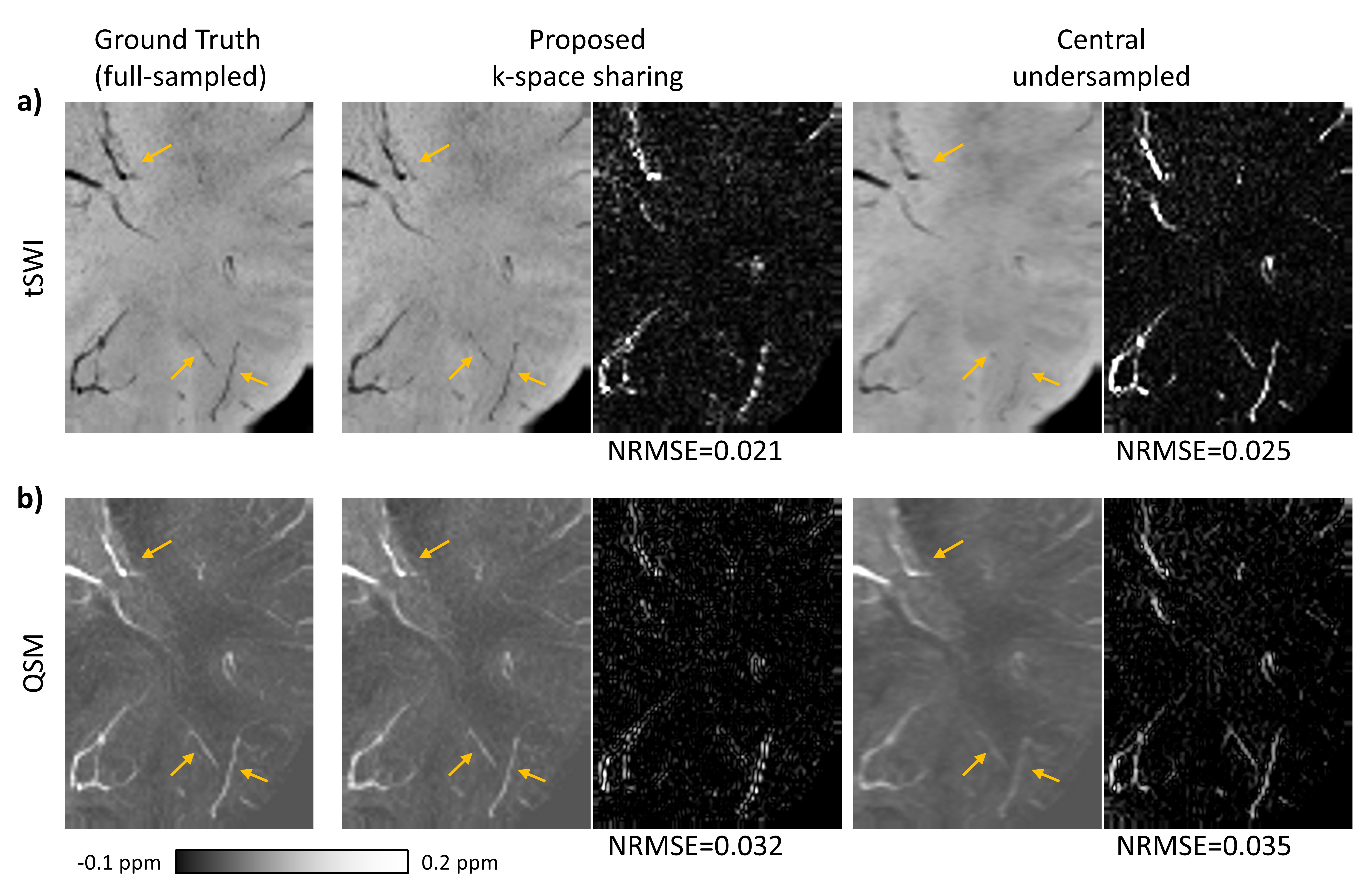
Data processing: STAGE data were processed in MATLAB using the methods described in references (7,8). For the exclusive high-resolution data, the two first echoes were centrally undersampled in k-space, while the two second echoes were merged into one k-space by the strategy shown in Figure-1. A Kaiser window filter with a beta of 2.0 was used on the central undersampled k-space data to reduce Gibbs rings generated by undersampling. For comparison purposes, the second echo of the low FA scan was centrally undersampled in the same way. Then, the three sets of SWI and QSM data (from fully-sampled data acting as ground truth (GT), proposed k-space sharing (IM1), and the central undersampled (IM2)) were compared visually, and by using a voxel based normalized root mean square error (NRMSE), NRMSEi=sqrt((GT-IMi)^2/(GT^2)). A brain mask generated from the QSM reconstruction (7) was used for the NRMSE calculation. The NRMSE number for each image was the average of those from all voxels in the whole volume.
Results
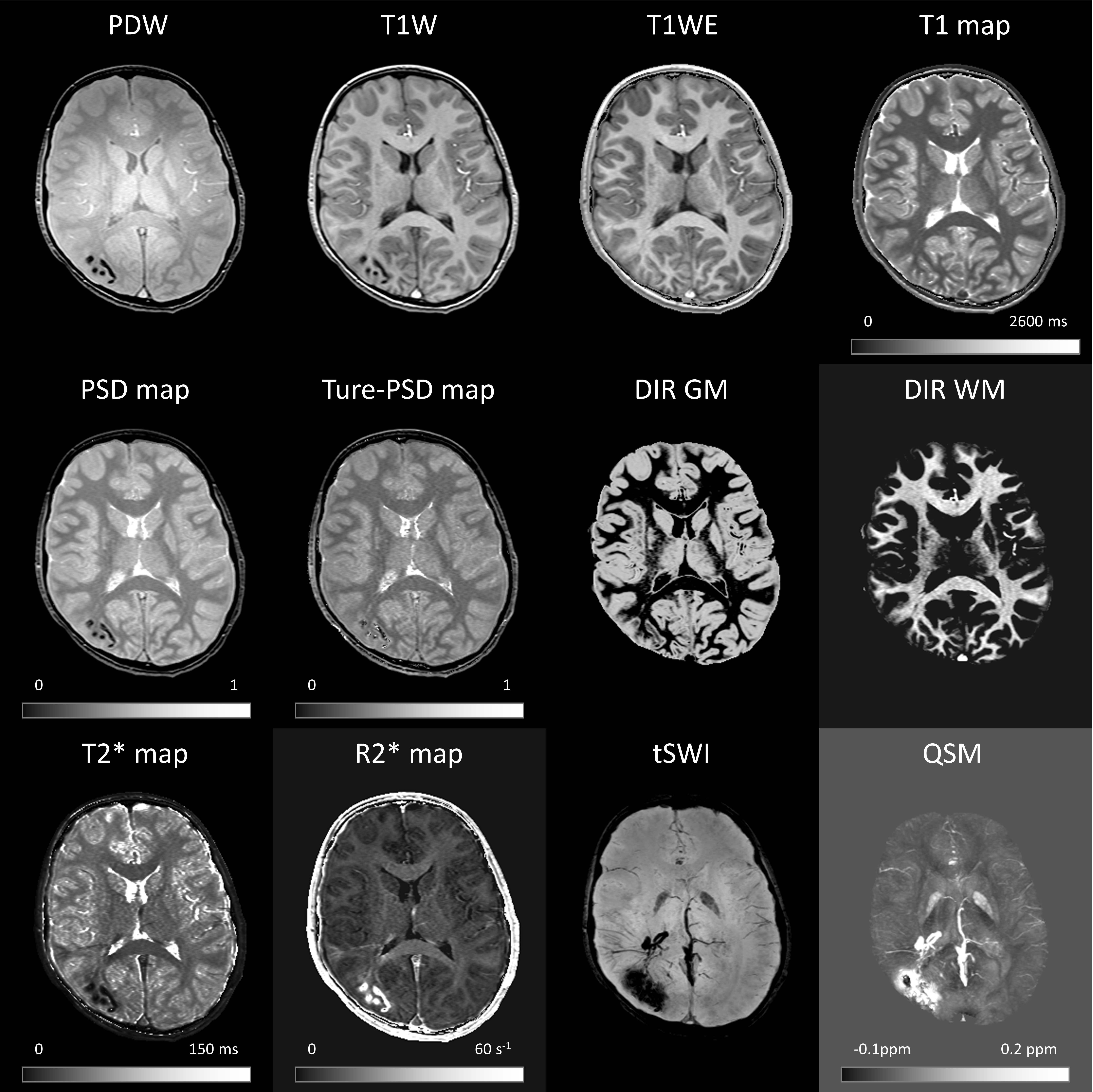
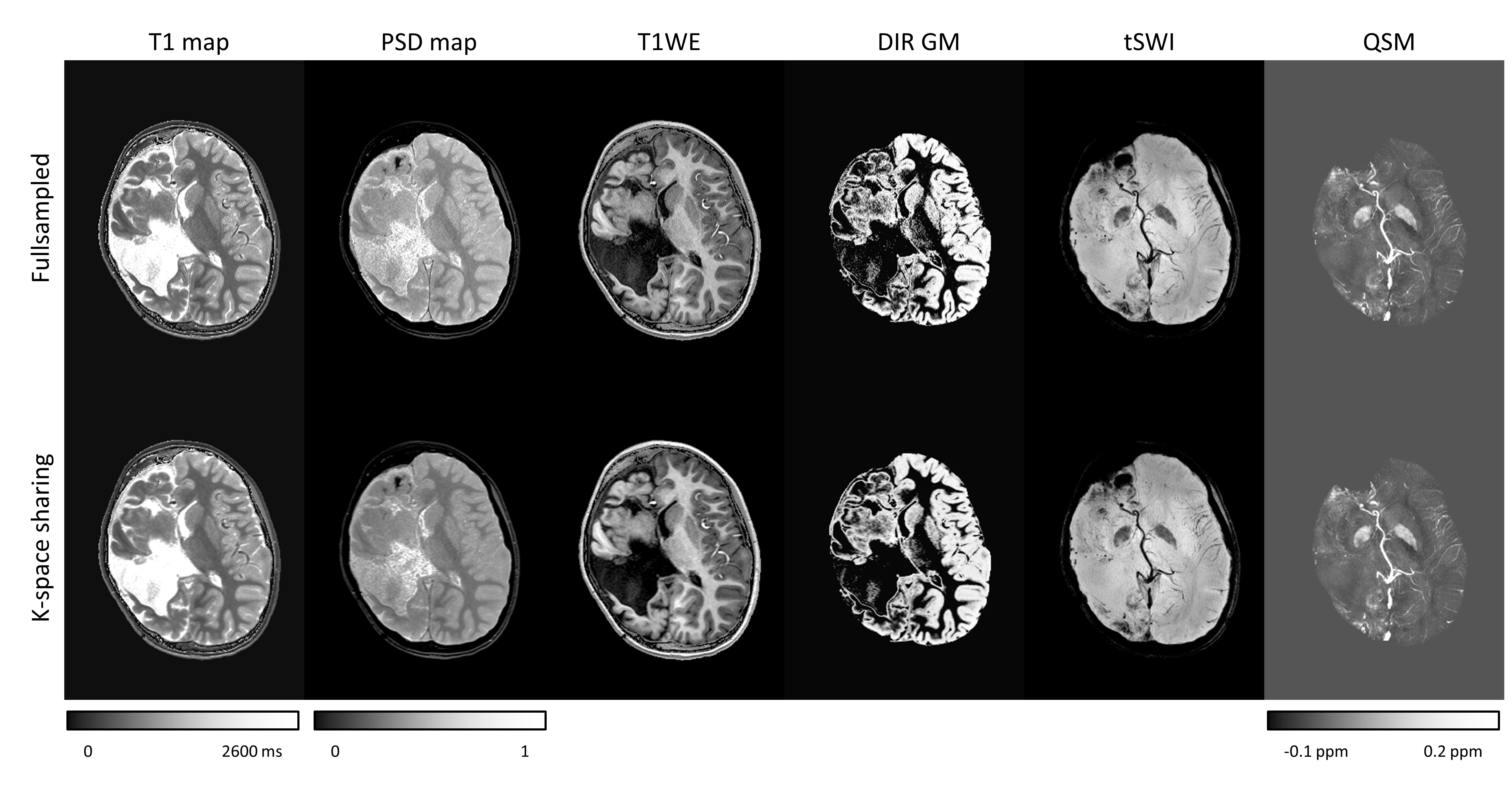
STAGE produced multiple qualitative and quantitative information from a 5-minute scan, including structural image contrasts, double inversion recovery (DIR) images, conventional SWI, true-SWI (or tSWI), as well as T1, T2* and susceptibility (Figure 2). Retrospective SWI and QSM results of the proposed k-space sharing strategy were visually close to the high-resolution ground truth (Figures 3 and 4) and much better than the central undersampled data. SWI and QSM images had lower NRMSE values (0.021, 0.032) than the central undersampled results (0.025, 0.035).Discussion and Conclusion
The current study was conducted retrospectively on fully-sampled data. Preliminary results from this analysis suggest this k-space sharing strategy for STAGE can provide enhanced resolution for SWI and QSM data. This approach still needs to be incorporated into a specialized sequence and online reconstruction used to prospectively evaluate this method in different pediatric neural situations. In summary, STAGE provides more than 10 pieces of information from just one 5-minute scan, including the high-resolution SWI and QSM results discussed herein, as well as high-SNR T1W, PDW, T1, PSD, and T2* mapping.Acknowledgements
The studies were supported by a grant from the NIH/NINDS (R01 NS41922).References
1. Vannest J, Rajagopal A, Cicchino ND, et al. Factors determining success of awake and asleep magnetic resonance imaging scans in nonsedated children. Neuropediatrics 2014;45:370–377.
2. Barkovich MJ, Xu D, Desikan RS, Williams C, Barkovich AJ. Pediatric neuro MRI: tricks to minimize sedation. Pediatr. Radiol. 2018;48:50–55.
3. Pan J, Quon JL, Johnson E, Lanzman B, Chukus A, Ho AL, Edwards MSB, Grant GA, Yeom KW. Rapid-sequence brain magnetic resonance imaging for Chiari I abnormality. J. Neurosurg. Pediatr. 2018:1–7.
4. Heathcock J, Hager L, Smith M. Feasibility of non-sedation MRI scans. Pediatr. Radiol. 2011;41:S371–S372.
5. Jaimes C, Gee MS, C. J, M.S. G. Strategies to minimize sedation in pediatric body magnetic resonance imaging. Pediatr. Radiol. 2016;46:916–927.
6. Hu J, Yu Y, Juhasz C, Kou Z, Xuan Y, Latif Z, Kudo K, Chugani HT, Haacke EM. MR susceptibility weighted imaging (SWI) complements conventional contrast enhanced T1 weighted MRI in characterizing brain abnormalities of Sturge-Weber syndrome. J. Magn. Reson. Imaging 2008;28:300–307.
7. Chen Y, Liu S, Wang Y, Kang Y, Haacke EM. STrategically Acquired Gradient Echo (STAGE) imaging, part I: Creating enhanced T1 contrast and standardized susceptibility weighted imaging and quantitative susceptibility mapping. Magn. Reson. Imaging 2018;46:130–139.
8. Wang Y, Chen Y, Wu D, Wang Y, Sethi SK, Yang G, Xie H, Xia S, Haacke EM. STrategically Acquired Gradient Echo (STAGE) imaging, part II: Correcting for RF inhomogeneities in estimating T1 and proton density. Magn Reson Imaging 2018;46:140–50.
Figures