3019
Detection of abnormal cortical morphology in children and adolescence with intermittent exotropia by anatomic magnetic resonance imaging1Department of Ophthalmology, West China Hospital, Sichuan University, Chengdu, China, 2Huaxi MR Research Center (HMRRC), Department of Radiology, West China Hospital, Sichuan University, Chengdu, China, 3Department of Optometry and Visual Science, West China Hospital, Sichuan University, Chengdu, China
Synopsis
The current study used anatomic magnetic resonance (MR) imaging to evaluate cortical structure alterations, age-related cortical and structural co-variance differences between children with intermittent exotropia (IXT) and healthy controls. The morphologic changes in the visual cortex and associations cortices, different anatomical-age correlation, and abnormal structural co-variance were detected in IXT group. These findings suggest possible disruptions of the cortical visual networks and the cortical maturation in IXT.
Purpose
Intermittent exotropia (IXT) is a common form of children strabismus, characterizedby intermittent divergent misalignment and binocular vision (e.g., stereopsis) impairment, and its incidence ranging from 1% to 3.24% in different countries1,2. Previous studies have reported brain structure and function changes in exotropic animals.3-5However, the neural substrates associated with IXT in humans remain unclear, and little is known about whether there are abnormities in cortical morphometric changes related to age, or structural co-variance alterations among brain regions of IXT. In present study, we used anatomic magnetic resonance (MR) imagingto investigate cortical differences, age-related cortical differences and structural co-variance differences between children with IXT and healthy control (HC).Method
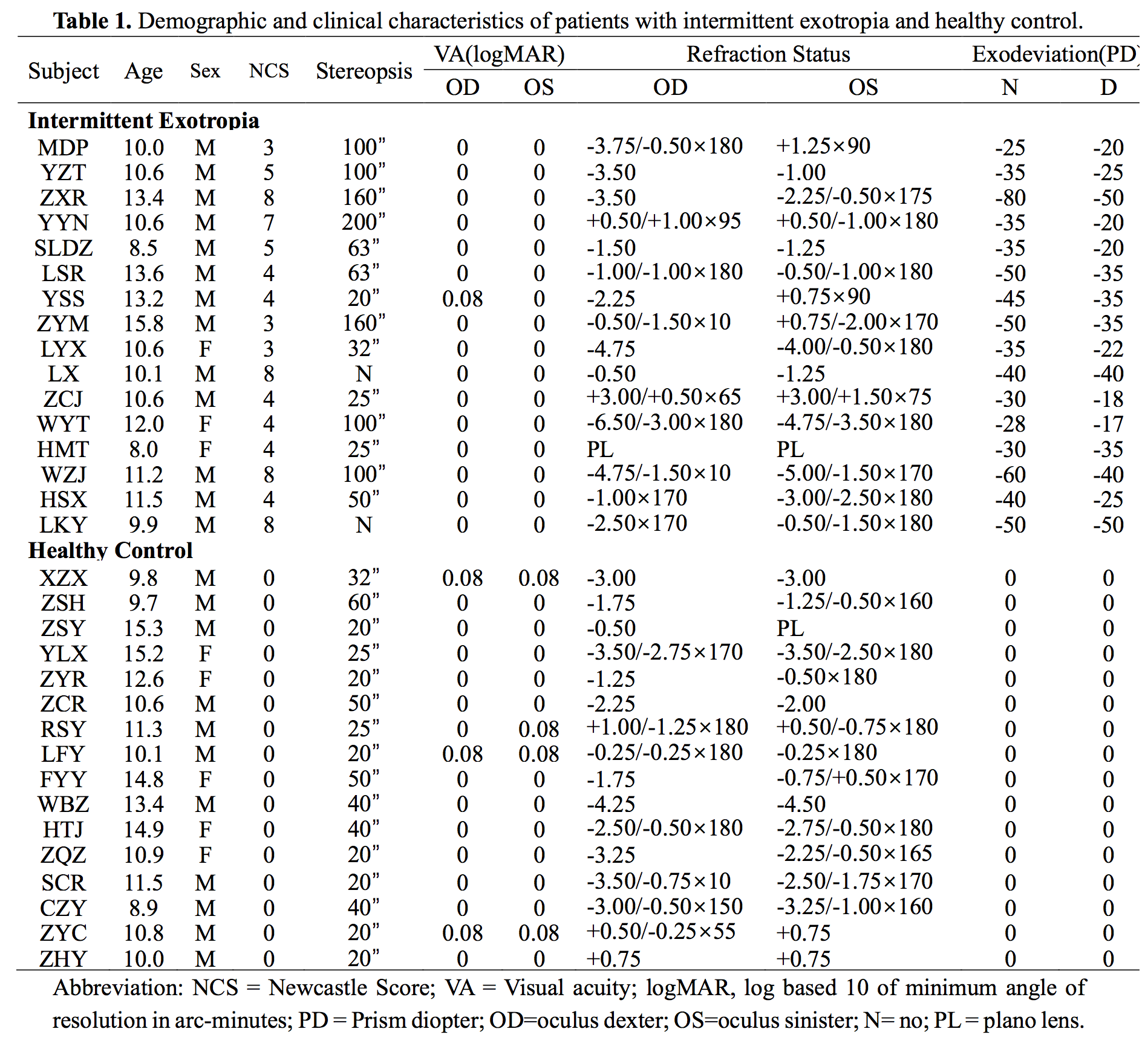
This prospective study was approved by the local ethical committee, and written informed consent was obtained from parents. Sixteen IXT patients and 16 age- (IXT = 11.23 ± 2.00; HC = 11.86 ± 2.20; P = 0.397), sex-, handedness-, education- matched healthy controls were recruited.Demographic and clinical characteristics of the IXT patients and HC are presented in Table 1. All subjects completed ocular examinations, including visual acuity, cycloplegic refraction, angle of deviation measured by prism and alternate cover test, stereoacuity, and exotropia control using the Newcastle Control Score. All participants were scanned using a 3-T MR scanner with an eight-channel phased-array head coil. High-resolution anatomical MR images were obtained with a spoiled gradient recalled sequence with the following parameters: repetition time/echo time, 2250 msec /2.62 msec; flip angle, 9°; section thickness, 1 mm; sagittal plane of acquisition, 192 slices; no slice gaps; field of view, 256×256 mm2; and voxel size, 1×1×1 mm3. FreeSurfer software was used to obtain measures of cortical volume, thickness, and surface area. Group differences in cortical thickness, volume and surface area were examined on the surface maps vertex by vertex, using a general linear model with the intracranial volume, age and sex as covariates. The age-related cortical differences between two groups were examined on the whole brain. Then, the structural co-variance of abnormal morphometric changes was examined. A Monte Carlo simulation with 10,000 iterations was used to control for multiple comparisons.The significance level was set at P< 0.05.Results
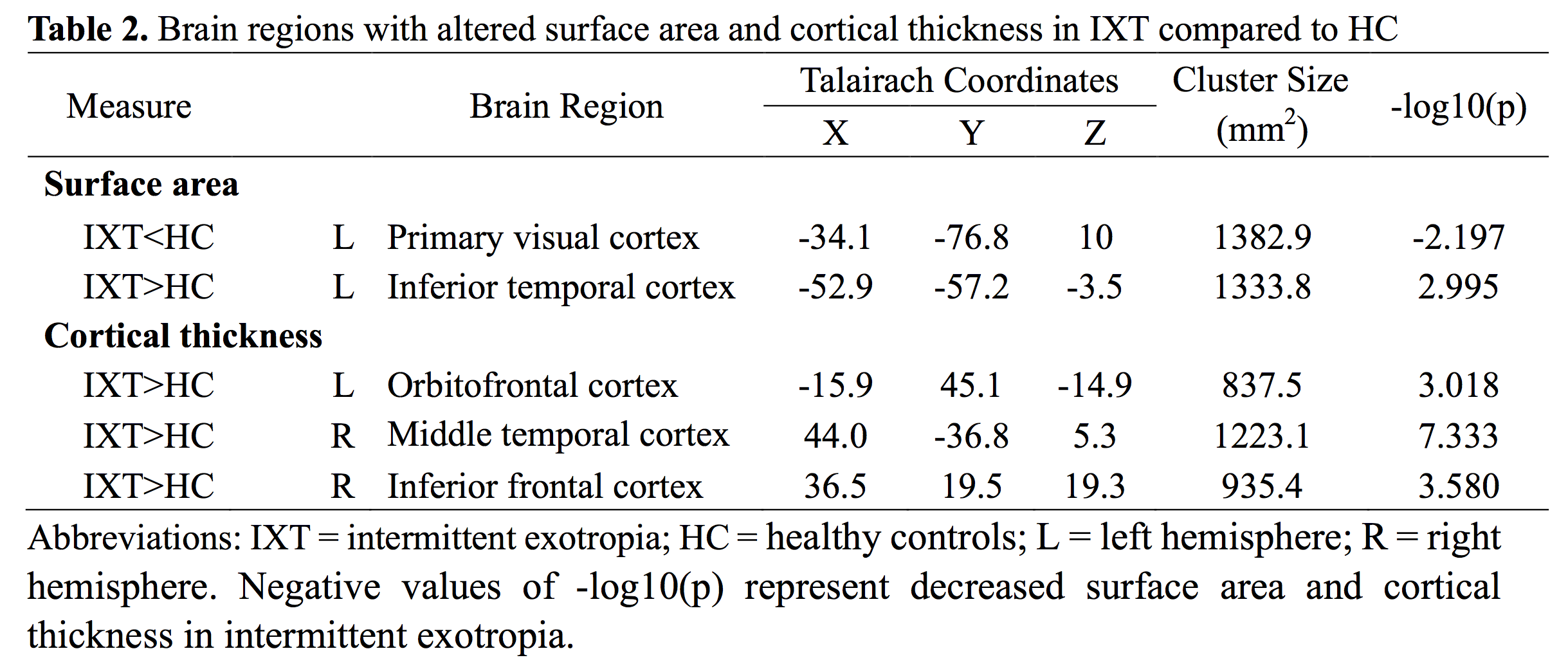
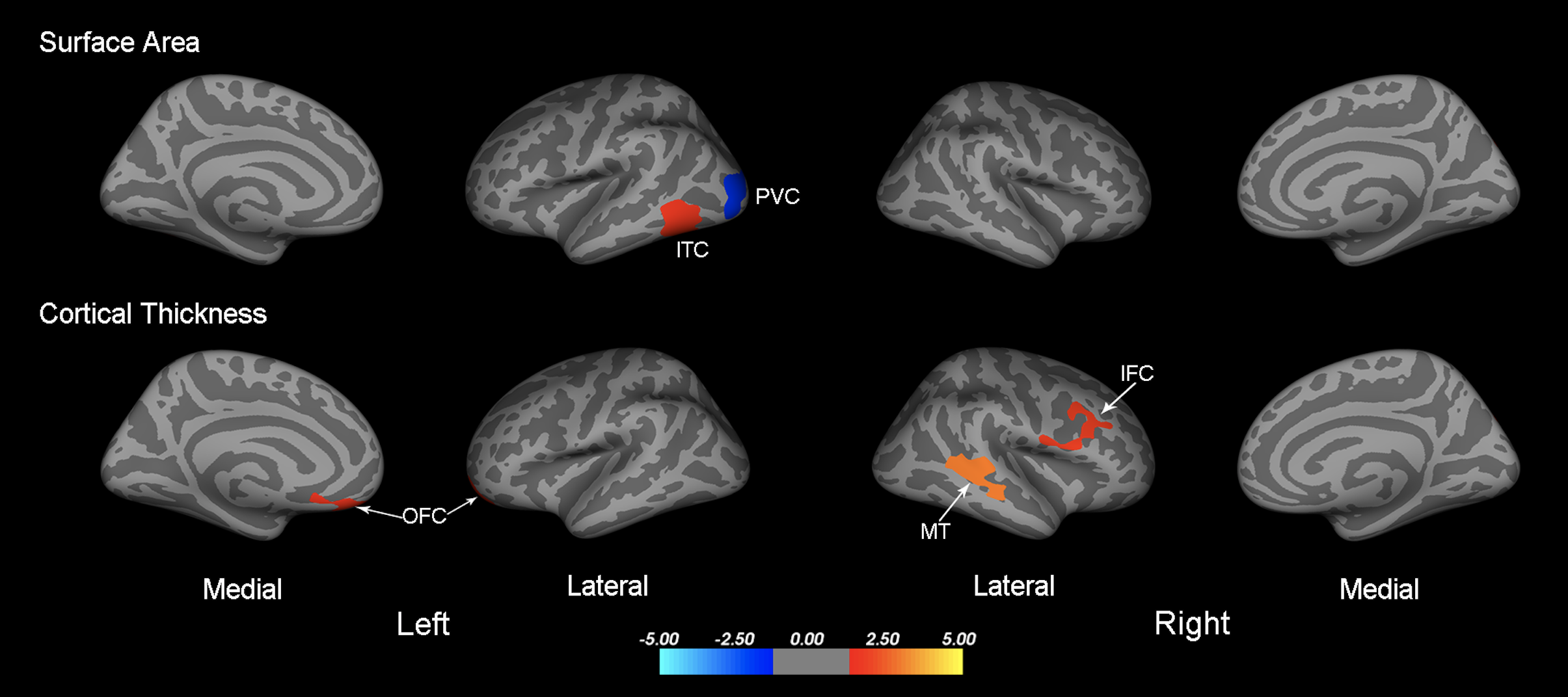
Compared to healthy controls, IXT patients demonstrated significantly decreased surface area in left primary visual cortex, and increased surface area in left inferior temporal cortex (Table 2; Figure 1). We also found increased cortical thickness in left orbitofrontal cortex, right middle temporal cortex, and right inferior frontal cortex (Table 2; Figure 1). No significant differences were found in cortical volume between the two groups.
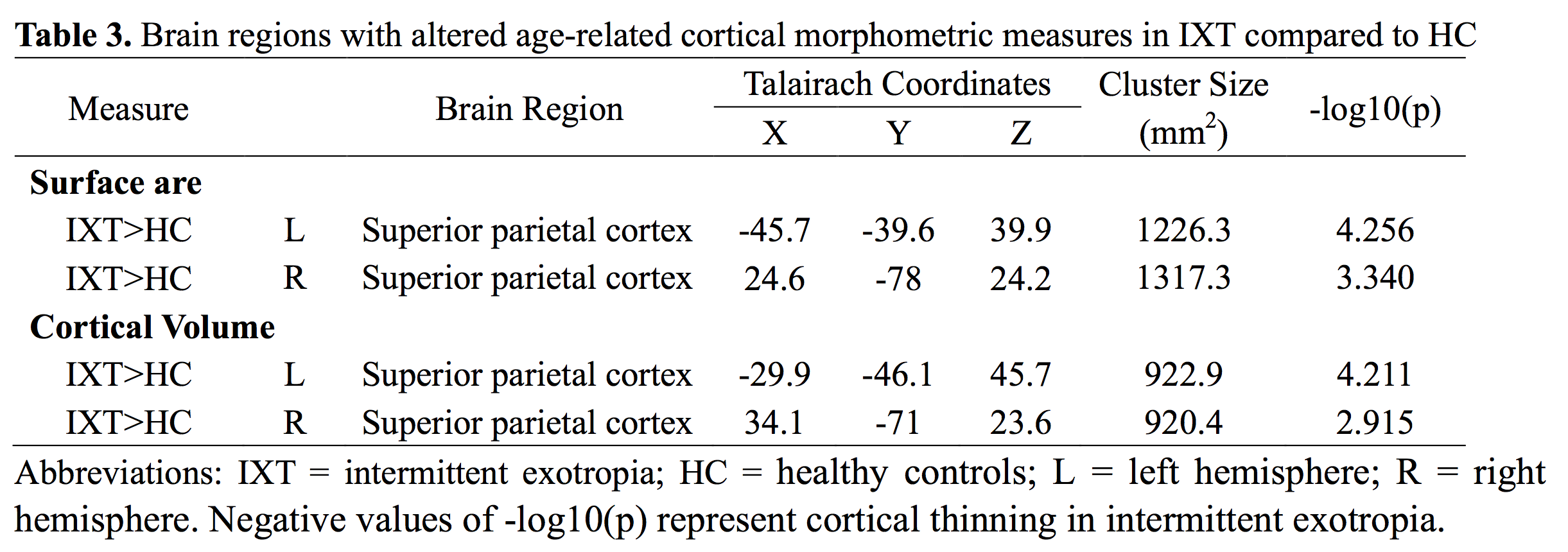
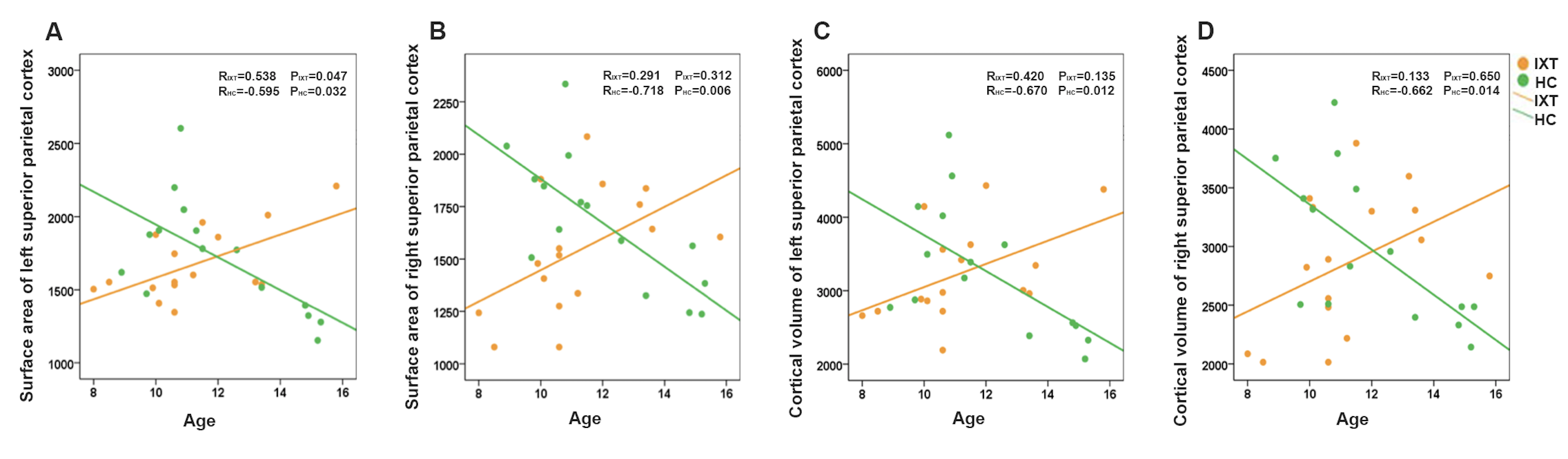
We found group differences in correlations between age and cortical morphometric measures in the superior parietal cortex (SPC). To show the age-related changes in SPC in each group, we extracted morphometric data of this region, and then performed correlation analyses. In the HC group, age was negatively correlated with surface area and cortical volume in left and right SPC (Table 3; Figure 2). However, in the IXT group, age was only positively correlated with surface area in left SPC (r = 0.538, P = 0.047) (Table 3; Figure 2A). No significant correlations between age and the other morphometric measures in SPC were observed in the IXT group (Figure 2B, 2C, 2D).
We also identified altered patterns of structural correlations across brain regions in patients with IXT. There were widespread significantly positive structural correlations between surface area and cortical volume in left and right SPC in the HC group (P< 0.05). In contrast, only the correlations between surface area and cortical volume of the ipsilateral SPC were significant in the IXT group (left SPC: r = 0.820, P < 0.001; right SPC: r = 0.830, P <0.001). A directly statistical comparison of correlation coefficients for the two groups demonstrated that the correlation between cortical volume of left and right SPC in the IXT group was significantly less than that in the HC group (z = 2.066, P < 0.05).
Conclusion
In the present study, we detected morphologic changes in the visual cortex and association cortices of human subjects with IXT. In addition, we also found different cortical morphometric development patterns in IXT group. Normal structural co-variance in the healthy control was disrupted in patients with IXT. These findings suggest possible disruptions of the cortical visual networks and the cortical maturation result from this special visual disorder.Acknowledgements
No acknowledgement found.References
1. Govindan M, Mohney BG, Diehl NN, et al. Incidence and types of childhood exotropia: a population-based study. Ophthalmology 2005; 112 (1): 104-108.
2. Pan CW, Zhu H, Yu JJ, et al. Epidemiology of Intermittent Exotropia in Preschool Children in China. Optom Vis Sci 2016; 93 (1): 57-62.
3. Sengpiel F, Jirmann KU, Vorobyov V, et al. Strabismic suppression is mediated by inhibitory interactions in the primary visual cortex. Cereb Cortex 2006; 16 (12): 1750-1758.
4. Adams DL, Economides JR, Sincich LC, et al. Cortical metabolic activity matches the pattern of visual suppression in strabismus. J Neurosci 2013; 33 (9): 3752-3759.
5. Scholl B, Tan AY, Priebe NJ. Strabismus disrupts binocular synaptic integration in primary visual cortex. J Neurosci 2013; 33 (43): 17108-17122.
Figures