3015
Elevated serum inflammation-related cytokines predict longitudinal changes of white matter integrity in mild traumatic brain injury1Medical Imaging, The First Affiliated Hospital of Xi’an Jiaotong University, Xian, China, 2The Key Laboratory of Biomedical Information Engineering, Ministry of Education, Department of Biomedical Engineering, School of Life Science and Technology, Xi'an Jiaotong University, Xi'an, China, 3Neurosurgery, The Second Affiliated Hospital and Yuying Children's Hospital of Wenzhou Medical University, Wenzhou, China, 4Radiology, The Second Affiliated Hospital and Yuying Children's Hospital of Wenzhou Medical University, Wenzhou, China, 5Center for Translational Medicine, The First Affiliated Hospital of Xi’an Jiaotong University, Xian, China, 6Psychiatry & Neuroscience, Center for Neuroproteomics and Biomarkers Research, University of Florida, Gainesville, FL, United States
Synopsis
Mild traumatic brain injury (
Purpose
The diffuse axonal injury is a major pathological hallmark of mild traumatic brain injury (mTBI) and leads to disruptions of white matter (WM) tracts associated with their poor clinical outcomes. 1-4 Diffusion tensor imaging (DTI) findings indicate the integrity of many tracts (i.e.the splenium of the corpus callosum) can predict clinical outcome after TBI.5 It is still unclear which factors contribute to such wide disruptions in WM after mTBI. Furthermore, numerous studies have characterized cytokines profiles and linked these elevated cytokines with adverse events and poor global outcomes after moderate to severe TBI. 6 Cytokines such as chemoattractant protein-1 (CCL2-MCP-1), interleukin-1β (IL-1β) and IL-6 propagate the inflammatory response and promote the neurotoxicity via excitotoxicity and oxidative injury after a traumatic impact. 7, 8 The present study aims to examine the dynamic association between WM integrity and inflammation-related cytokines in mTBI patients with longitudinal observations from 7 days to 3 months post-injury.
Methods
We assessed 33 mTBI patients within 7 days post-injury (T-1, acute phase) and follow-up at 1 month (T-2, sub-acute phase) and 3 months (T-3, chronic phase) respectively. 31 age, gender-matched healthy controls were enrolled. Measures included a 9-plex panel of serum cytokines and DTI. The independent two-sample t-test and the Mann-Whitney test were used to compare group differences based on data normality, respectively. Chi-square analyses were applied to assess categorical variables. Longitudinal analysis was conducted to examine changes in both cytokines and imaging Fractional anisotropy (FA) metric as a function of recovery. In a factorial model, main effects of group and time, as well as a group by time interaction were examined. Spearman’s correlation coefficient was used to examine the association between cytokines and FA over different phases. The significance level was adjusted by using the family-wise Bonferroni correction with P < 0.05.
Results
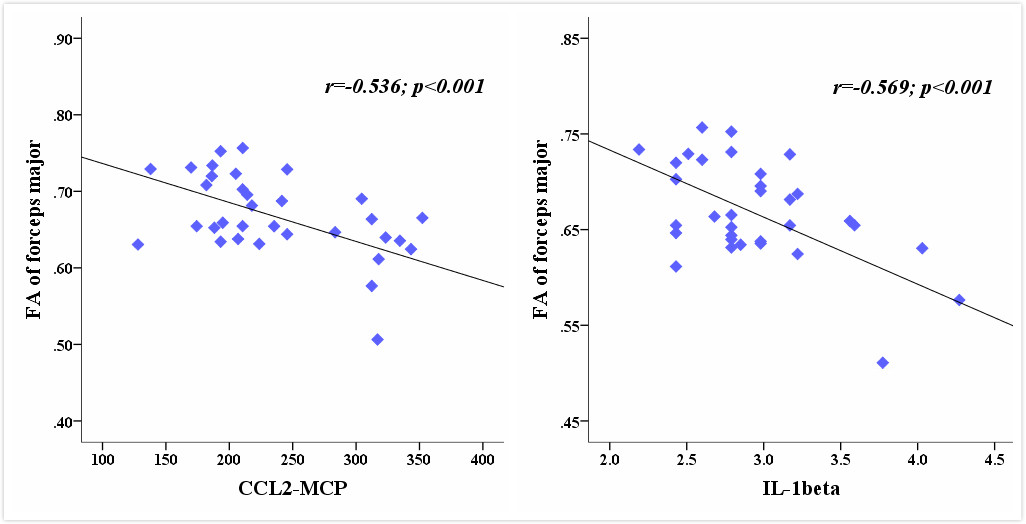
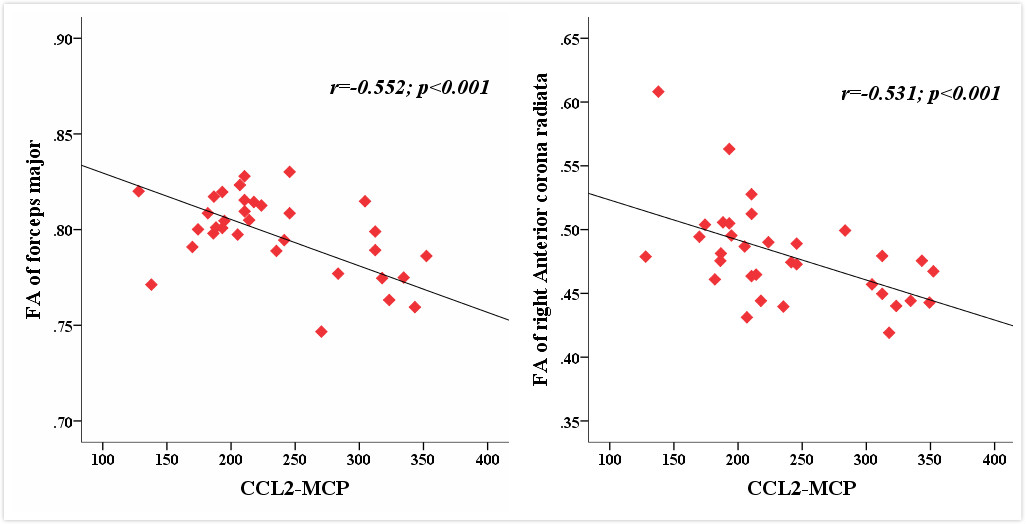
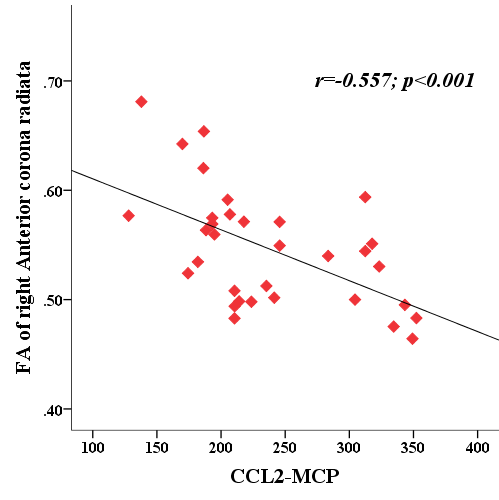
MTBI patients showed significant increases in the CCL2-MCP-1, IL-1β and IL-6 across all time points compared with controls (all P < 0.001). Longitudinal analyses indicated a significant effect of time for these three cytokines (all for P < 0.02). CCL2-MCP-1 exhibited persistently increased at both T-2 (P < 0.001) and T-3 (P < 0.001) compared with T-1 while the other two showed decreased at T-3 compared with T-1. For DTI, there was no significant interaction effect. Significant main effect of time was located in the left anterior limb of internal capsule (ALIC), right inferior fronto-occipital fasciculus (IFOF) and body of corpus callosum (CC) (all for P < 0.005). The left ALIC and right IFOF returned to the normal level at both T-2 and T-3, while the body of CC exhibiting continuing loss across all time points (P < 0.001).There were also some tracts (right anterior corona radiate, ACR; forceps major) with significant loss of integrity only at later T-2 and T-3 periods (all for P < 0.002). Correlation analysis further indicated that elevate CCL2-MCP-1 and IL-1β were associated with the decreased FA in the forceps major (r = -0.536, P < 0.001; r = -0.569, P < 0.001) at T-1 (Fig. 1). CCL2-MCP-1 at T-1 was also shown negative correlation with FA values in the forceps major and right ACR at T-2 (r = -0.552, P< 0.001; r = -0.531; P< 0.001) (Fig. 2). The initial level of the CCL2-MCP-1 can also predict the loss of structural integrity in the right ACR at T-3 (r = -0.557, P < 0.001) (Fig. 3).
Discussion
The present study found that cytokines in serum presented significant increases within 7 days post-injury and persisted beyond 3 months following mTBI. Particularly, the increased CCL2-MCP-1 at acute phase can partly explain the continuing WM damages in the forceps major and right ACR at during 1 or 3 month post-injury. The forceps major is located in the splenium of CC and its corresponding functional projection area is mainly located in the combined area of the occipital-parietal-temporal lobes. Damage in this area may affect a variety of cognition recovery. In addition, the ACR is part of the limbic-thalamo-cortical circuitry and includes thalamic projections to the prefrontal areas that have been associated with impaired top-down emotion regulation systems.
Conclusion
Our results reflected the association of inflammatory cytokines at the early acute period with the continuing WM fiber damages in the later recovery period. The finding had the potential clinical significance and suggested an early intervention on the inflammatory cytokines in order to decrease the structural integrity loss in the WM tracts.
Acknowledgements
The authors report no conflicts of interest.References
1. Gentleman SM, Roberts GW, Gennarelli TA, et al. Axonal injury: a universal consequence of fatal closed head injury? Acta Neuropathol. 1995;89(6):537–543.
2. Ham TE & Sharp DJ. How can investigation of network function inform rehabilitation after traumatic brain injury? Curr Opin Neurol. 2012;25(6):662–669.
3. Sharp DJ, Scott G & Leech R. Network dysfunction after traumatic brain injury. Nat Rev Neurol 2014;10(3):156–166.
4. Hellyer PJ, Leech R, Ham TE, et al. Individual prediction of white matter injury following traumatic brain injury. Ann Neurol 2013;73(4):489–499.
5. Amor S, Peferoen LA, Vogel DY, et al. Inflammation in neurodegenerative diseases--an update. Immunology. 2014;142(2):151-166.
6. Woodcock T & Morganti-Kossmann MC. The role of markers of inflammation in traumatic brain injury. Front Neurol. 2013;4:18.
7. Gyoneva S & Ransohoff RM. Inflammatory reaction after traumatic brain injury: therapeutic potential of targeting cell-cell communication by chemokines. Trends Pharmacol Sci. 2015;36(7):471-480.
8. Morganti-Kossmann MC, Satgunaseelan L, Bye N, et al. Modulation of immune response by head injury. Injury. 2007;38(12):1392-1400.
Figures