3011
White Matter Microstructural Change Following Traumatic Brain Injury Assessed by Biophysical Modeling using Simultaneous Multi-Slice Multi-Shell Diffusion MRI1National Intrepid Center of Excellence (NICoE), Walter Reed National Military Medical Center, Bethesda, MD, United States
Synopsis
Mild traumatic brain injury (mTBI) is difficult to diagnose and characterize. In this study, we applied simultaneous multi-slice multi-shell diffusion MRI to assess white matter microstructural changes in chronic military mTBI. Preliminary results showed parameters derived from diffusion MRI biophysical modeling are superior to the parameters derived from diffusion tensor imaging in differentiating tissues with distinct structural and architectural features, and thus has increased ability to identify microstructural changes in mTBI.
Introduction
Mild traumatic brain injury (mTBI) is difficult to diagnose and characterize. Identifying underlying aberrant white matter (WM) structural changes associated with persistent post-concussive symptoms can differentiate mTBI from purely psychological disorders. Advanced diffusion MRI (dMRI) techniques using biophysical modeling show promising results in assessing brain tissue microstructure. Specifically, multi-compartment microscopic diffusion anisotropy imaging yields estimates of microscopic features specific to the intra- and extra-neurite compartments in nervous tissue and are not confounded by the effects of orientation dispersion and fiber crossings1,2,3. In this study, we assessed microstructural changes in chronic military mTBI patients by applying biophysical models to dMRI acquired with a simultaneous multi-slice (SMS) multi-shell sequence.Method
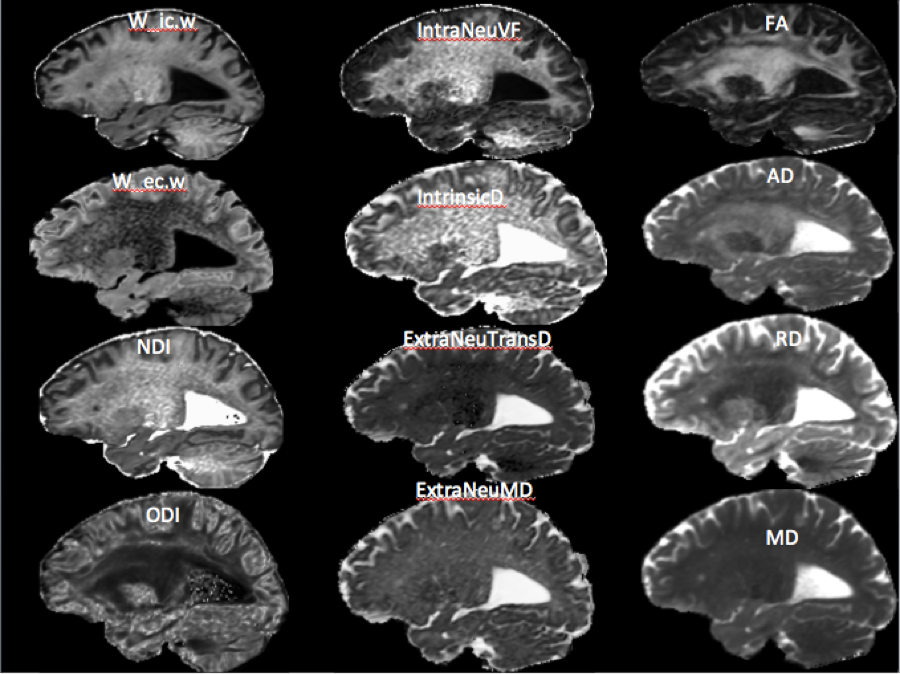
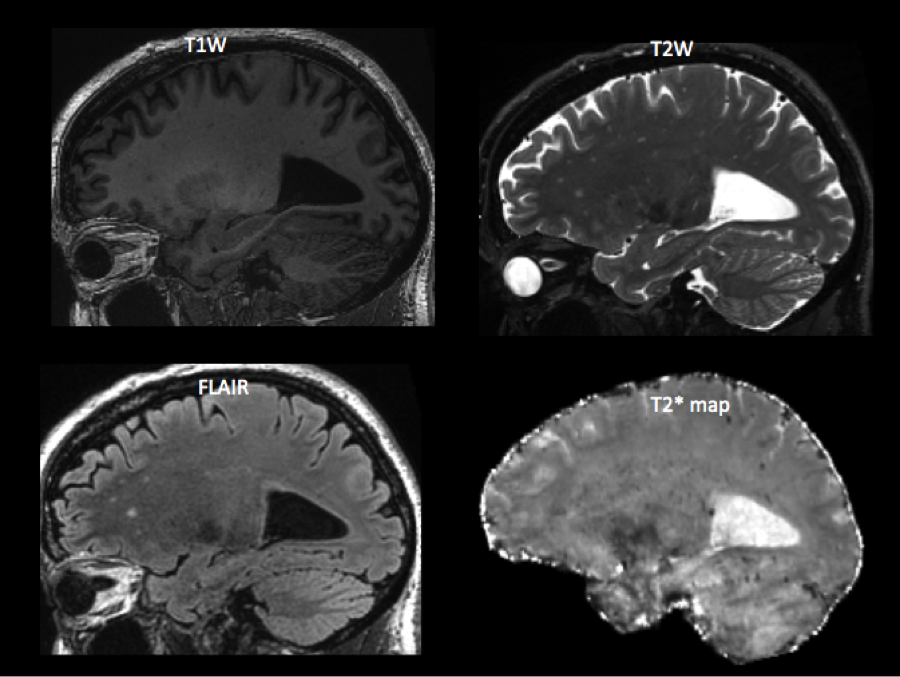
One hundred and twenty (120) male service members (age: 40.18 ± 5.88 years old) previously diagnosed with mTBI received a series of neuroimaging exams at the National Intrepid Center of Excellence using a 3T scanner equipped with a 32-channel head coil. Twenty-two (22) non-TBI male control subjects were recruited for comparison (age: 35.50 ± 8.64 years old). SMS multi-shell diffusion MRI was acquired in about 25 minutes using sparse and optimal acquisition schemes4 with three shells (b=1000, 2000, 3000, 1.7 mm3) and a SMS acceleration factor of three. First, data were preprocessed with noise reduction, motion eddy current correction and non-linear registration to the structural T2W image using the TORTOISE package5. Then microstructural changes in chronic mTBI patients were detected by applying two biophysical models: 1) Neurite Orientation Dispersion and Density Imaging (NODDI) metrics were reconstructed using a robust and fast nonlinear cascaded optimization algorithms (Maastricht Diffusion Toolbox6; and 2) a multi-compartment microscopic model using the Spherical Mean Technique7 (SMT) was computed. The reconstructed metrics include intra-cellular volume fraction (w_ic.w) and extra-cellular volume fraction (w_ec.w), neurite density index (NDI), and orientation dispersion index (ODI) estimated by using the Watson distribution on a cylindrical geometry (MDT NODDI) (left column in Fig. 1); and intra-neurite volume fraction (IntraNeuVF), intrinsic diffusivity (IntrinsicD), extra-neurite transverse diffusivity (ExtraNeuTransD), and extra-neurite mean diffusivity (ExtraNeuMD) (SMT) (middle column in Fig. 1). DTI-derived parameters, e.g. fractional anisotropy (FA), radial diffusivity (RD) and axial diffusivity (AD) and mean diffusivity (MD) (right column in Fig. 1) were also estimated. In addition, the structural MRI, e.g. T1W, T2W and T2w FLAIR, susceptibility weighted imaging, and quantitative T2* maps were used to assess macrostructural changes, such as white matter hyperintensities (Fig. 2). Diffusion metrics were warped to MNI template using diffeomorphic nonlinear transformation and smoothed (at 5mm) for further voxel-wise analysis. General linear mixed modeling was applied to evaluate the difference of dMRI biophysical model derived parameters between non-TBI and mTBI subjects by modeling covariates of age. Significance was tested using non-parametric permutation test with TFCE (Threshold-Free Cluster Enhancement, Smith et al. 2016) as well as Monte Carlo simulations with 0.05 family-wise error (FWE) for correcting multiple comparisons of the whole brain voxel-wise analysis.Results
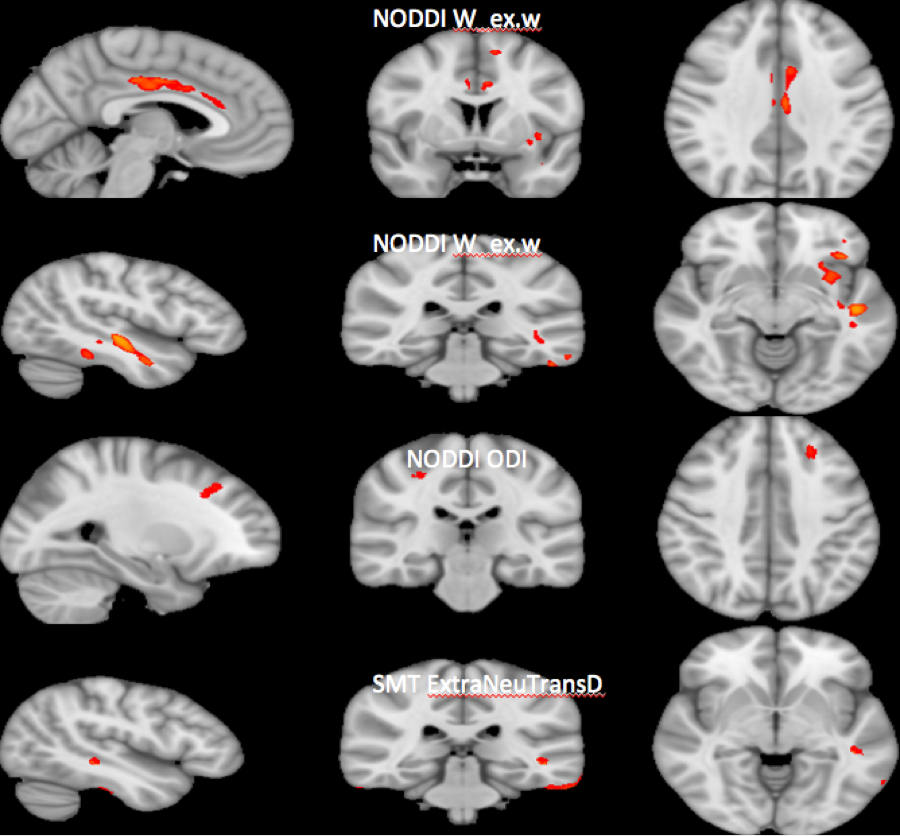
More than 90% of WMHs were located over the bilateral prefrontal regions (results not shown). Compared to non-TBI controls, the mTBI group had lower extra-cellular volume fraction over the bodies of bilateral cingulate, the left insular region and the left temporal region (FWE=0.05 using TFCE) (top and the 2nd row in Fig, 3), lower orientation dispersion index over the bilateral dorsolateral prefrontal region (Monte Carlo simulation,voxels > 45, using MDT NODDI) (3rd row in Fig. 3), and lower extra-cellular transverse diffusivity over the left insular region (Monte Carlo simulation,voxels > 45, using SMT) (bottom in Fig. 3). These clusters were mainly at the gray matter and white matter junctions. Lower extra-cellular volume fraction and lower extra-cellular transverse diffusivity around the gray insular region in mTBI but without NDI changes suggest reactive astrogliosis, glial scarring caused by chronic inflammation without axonal damage. These processes would result in lower hindered diffusion, i.e. decreased radial diffusivity8.Discussion and Conclusion
In this study, we have demonstrated the feasibility of applying advanced diffusion MRI techniques to identify WM microstructural changes related to mTBI. Our findings of lower extra-cellular volume fraction, lower extra-cellular transverse diffusivity, and lower white matter orientation dispersion index, particularly at the junctions of gray matter and white matter suggest chronic inflammation may play an important role in the long-term outcome of mTBI patients. In addition, our results showed dMRI biophysical modeling is more sensitive than DTI measures in assessing WM microstructural changes in mTBI. Since our non-TBI group was younger than the TBI group, age effects may contribute to these findings. This ongoing project will evaluate possible confounding effects using a larger sample size. These results suggest that SMS multi-shell dMRI biophysical metrics might be sensitive to white matter changes in chronic military mTBI. In conclusion, dMRI biophysical modeling may have applications in monitoring persistent post-concussive symptoms and brain recovery in chronic military mTBI patients.Acknowledgements
Disclaimer: The identification of specific products, scientific instrumentation, or organization is considered an integral part of the scientific endeavor and does not constitute endorsement or implied endorsement on the part of the author, DoD, or any component agency. Theviews expressed in this abstract are those of the authors and do not reflect the official policy of the Department of Army/Navy/Air Force, Department of Defense, or U.S. Government.References
1. Harms, R.L. et al. (2017) NeuroImage 155:82-96.
2. Kaden E. et al., (2016) NeuroImage, 139:346-3593.
3. Zhang, H. et al.; (2012) NeuroImage61(4):1000-1016.4.
4. Koay C.C. et al., (2012) MedicalPhysics.39(5), 2499-2511.
5. Pierpaoli, C. et al., (2010) ISMRM 18thAnnual Meeting (https://science.nichd.nih.gov/confluence/display/nihpd/TORTOISE).
6. Maastricht Diffusion Toolbox (https://github.com/cbclab/MDT).
7. Spherical Mean Technique (https://github.com/ekaden/smt).
8. Hutchinson, E.B. et al. (2018) J Neurosci Res.2018; 96(4):612-625.
Figures