3010
TBI-induced alterations in white matter microstructure relate to impairments in cognition and psychological functioning1Medical Physics, University of Wisconsin - Madison, Madison, WI, United States, 2Waisman Center, University of Wisconsin - Madison, Madison, WI, United States, 3Pediatrics, Univesity of Wisconsin - Madison, Madison, WI, United States, 4University of Wisconsin - Madison, Madison, WI, United States
Synopsis
Diffusion tensor imaging (DTI) was performed one-two years after severe traumatic brain injury in a cohort of pre-adolescent and adolescent children. The study investigated the relationships between DTI measures and variations in performance for memory and executive function, and overall clinical dysfunction. Mean diffusivity (MD) in the fornix correlated with learning and verbal tasks. MD in the corpus callosum and global white matter was related to global fuction.
Introduction
Traumatic brain injury in children is a significant cause of long-term disability. There is a critical need to better understand the relationships between brain networks as measured by MRI and clinical/behavioral outcomes. This study attempted to relate measures of white matter tract microstructure to specific clinical outcome and neurocognitive measures at 1-2 years following severe traumatic brain injury in a 35 children cohort ages 9-18 years. Specifically, the study investigated how white matter microstructure was affected in the following domains:
Default-Mode-Network(DMN): connects nodes within prefrontal-cortex, lateral-inferior-parietal-lobes, medial-temporal-lobes, and posterior-cingulate-cortex(PCC). The main tract connecting prefrontal structures and PCC is the cingulum. Dense interconnectivity between frontal and posterior DMN nodes is important for efficiently directing attention and switching between internally directed and task oriented cognitive processes1. TBI-induced alterations in DMN may cause impairments in executive function like decreased ability to monitor one’s engagement in goal-directed tasks, and may correlate with measures of task initiation, behavioral monitoring, and planning.
Hippocampal-Memory-Network(HMN): connects hippocampus, parahippocampus, and cortical hub nodes within other networks like pCC(DMN), andamygdala(Limbic). The fornix tract is core in connecting hippocampus and limbic system nodes.Injury to hippocampus or its major input/output pathways causes impairments in memoryencoding and retrieval. Memory and learning are frequently affected in children with TBI2.
Global-Network-Dysfunction: While up to 20% of children have impairments in only onefunctional domain after TBI, 40% have deficits in >2 domains3. Efficient cognitive functionrequires coordinated activity across multiple networks. Within the conceptual framework ofTBI-induced network dysfunction, while individual network disruption may be evidenced bydeficits within a specific domain, very severe or global injuries are expected to impact multiplenetworks resulting in impairments in global function.
Methods
TBI patient scans were collected across multiple centers/scanner types using a standardized imaging protocol, which included diffusion weighting (b=1300) along 64 non-colinear directions, 8 volumes with b=0, and 2.5mm isotropic resolution. 35 typically-developing controls(ages:9-18) were scanned at a single center.
Mean diffusivity (MD) was calculated for whole-brain-white-matter(GWM), corpus-callosum(CC), fornix, and cingulum, which were defined by corregistration to the IIT White Matter Atlas(v.4.1) using ANTs5.
Global function was assessed using the GOS-E-Peds6,7. Executive function and verbal memory were assessed with domain specific outcome measures using the Behavior Rating Inventory of Executive Function(BRIEF)8,9 and the California Verbal Learning Test(CVLT)10, respectively.
Ordinal-logistic-regression was used for investigating associations between MD and GOS-E-Peds global connectivity measures. Linear-regression was used for investigating associations between MD and BRIEF/CVLT domain specific outcome measures.
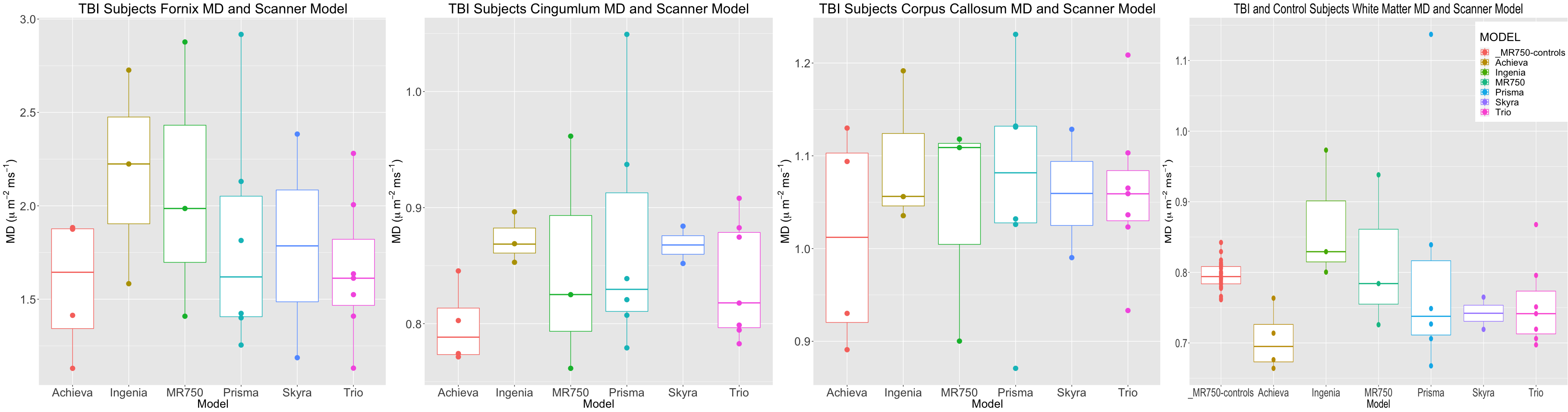
Age was controlled for in all regressions. In order to account for variability according to scanner type as seen in Figure-1, a scaling factor was computed by the ratio of white matter median MD over scanner type group to the median over all TBI subjects white matter MD. All of the MD values in the different regions were scaled by this ratio.
Results
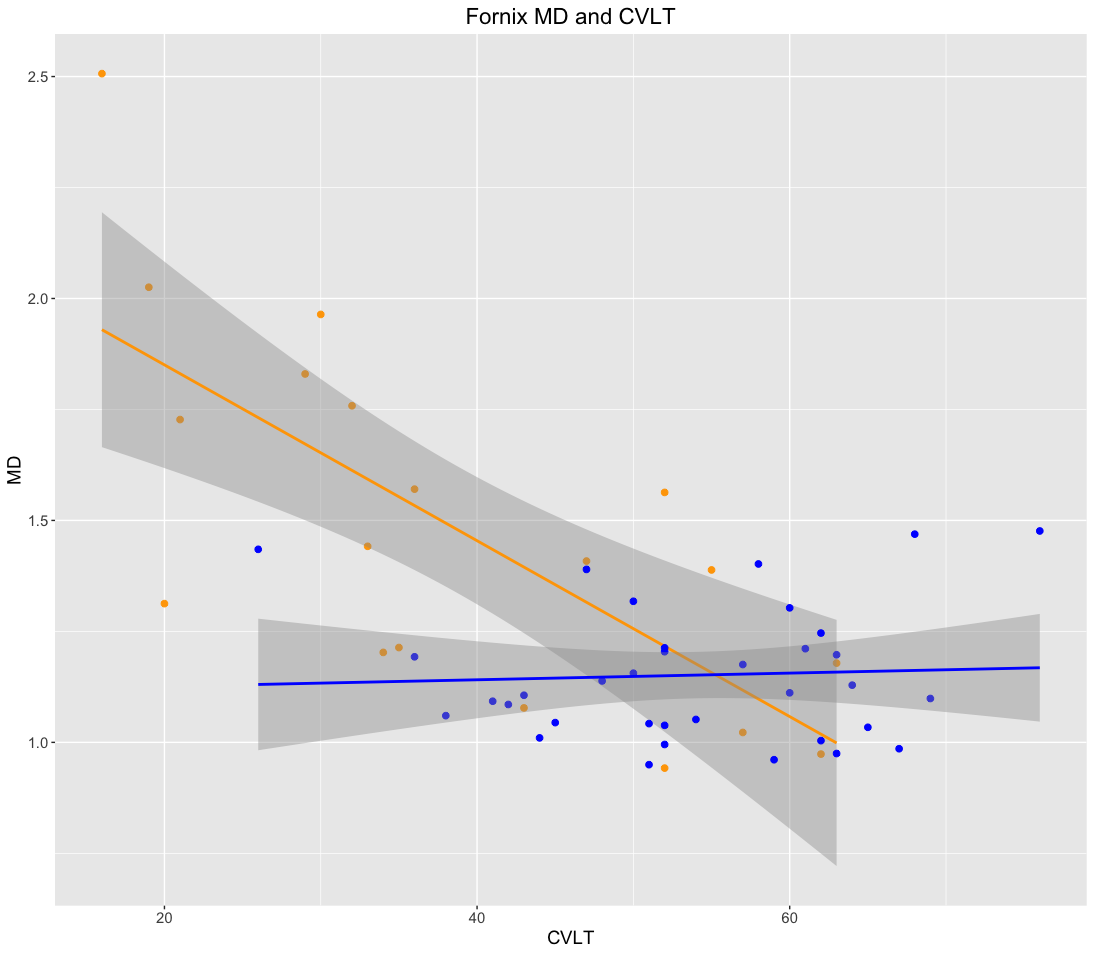
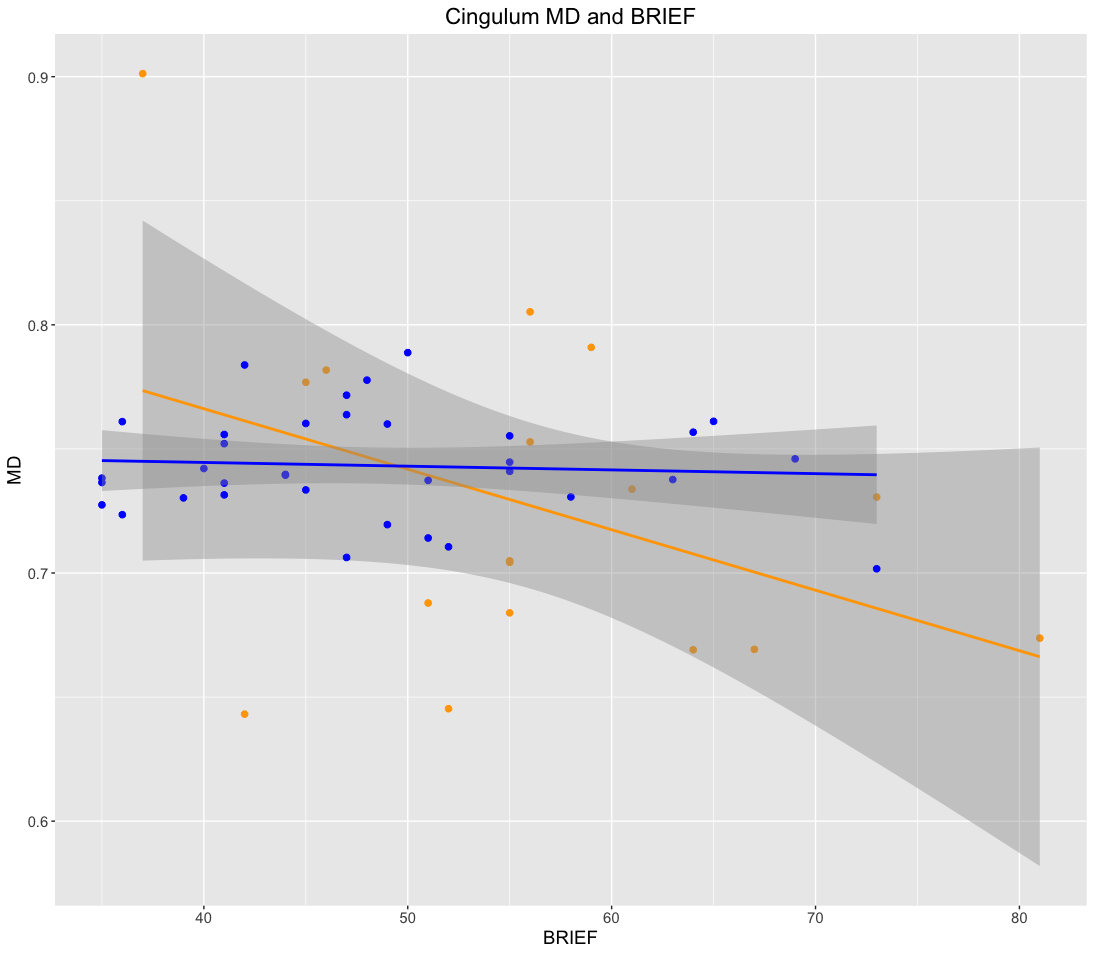
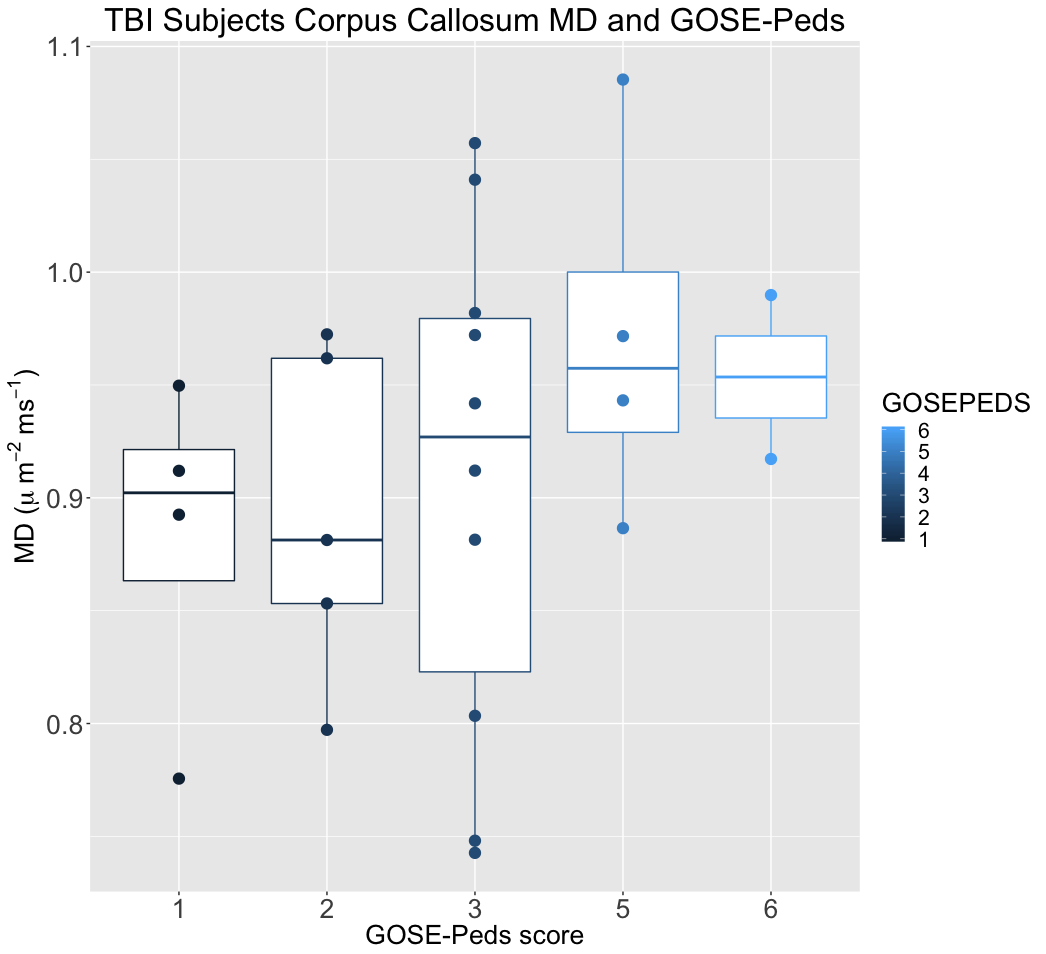
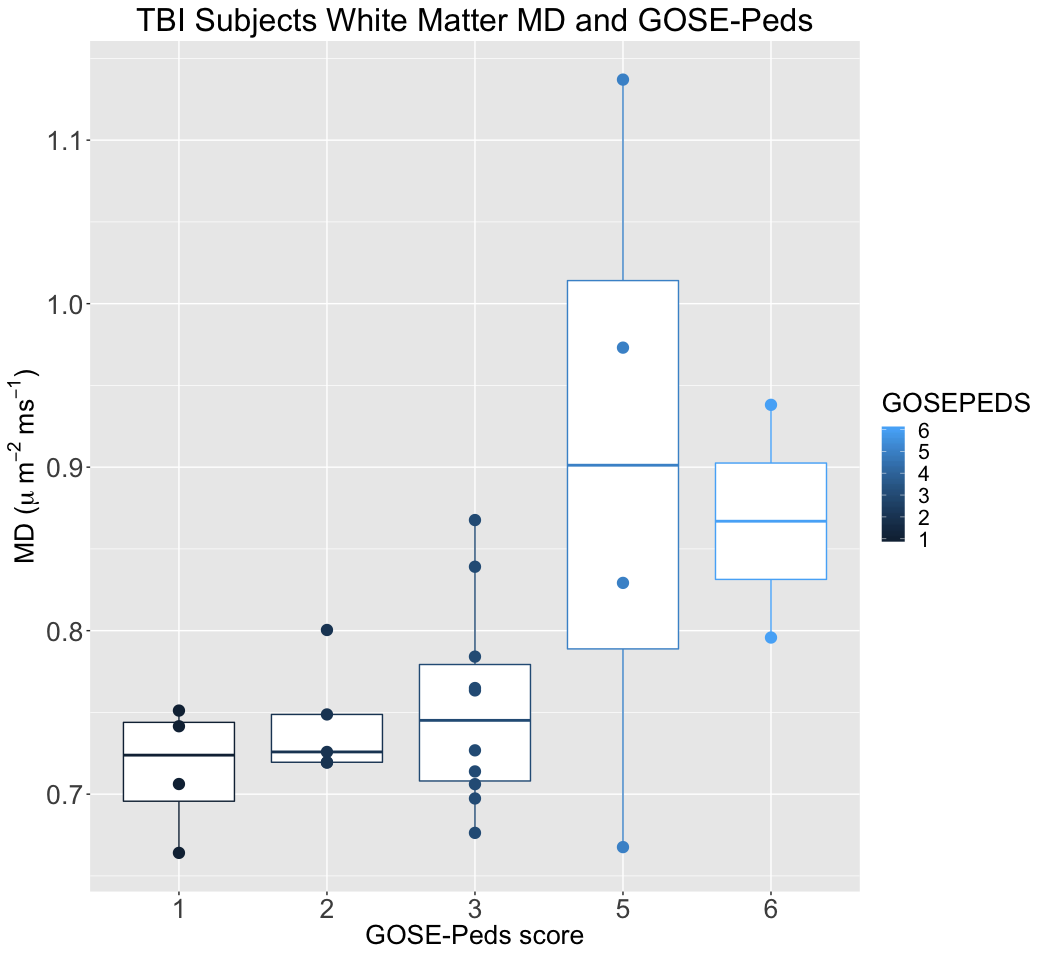
The graphs in Figures 2-5 demonstrate correlations between regional MD for the TBI group with the different outcome measures.
Multiple-comparisons-Boneferroni-adjusted p-values for the associations of MD in the fornix with CVLT and MD in the cingulum with BRIEF are p<0.0045 and p<0.49, respectively. Corrected p values for correlation of MD in the CC with GOS-E-Peds and GWM MD with GOS-E-Peds are p<0.61 and p<0.12, respectively.
No associations were found between outcome measures and MD for the control group.
Discussion
As expected, children with a prior history of severe TBI demonstrated differences in white matter microstructure. In addition, we observed several relationships between microstructural measurements in specific white-matter regions and domain-specific network measures.
The HMN findings are consistent with reduced hippocampal connectivity and CVLT impaired recall after TBI in an adult rfMRI study11. The CC and WM findings are consistent with a recent study which found CC FA correlated with impairments across multiple cognitive/psychological domains when comprehensive neuropsychological testing was performed after severe pediatric TBI12. They also support the view that CC injury is a marker of global network disruption.
The DMN findings, however, are a bit counterintuitive. Figure-3 associates lower MD with poor executive function, contrasting with recent TBI studies where cingulum tract disruption correlated with reaction-time on cognitive control measures13 and executive function impairments14. One can speculate on our findings that because cingulum fibers are atrophied as a result of injury, any remaining fibers in the bundle adapt to compensate for lost fibers leading to higher integrity in those remaining fibers. Note, too, that most of the TBI subjects did not demonstrate clinical impairment on the BRIEF measures (i.e. only 3 subjects had clinical significant BRIEF score >65). On the other hand, one cannot discard site effects driving some of the observed associations. This last item is the subject of current and future work.
Acknowledgements
Support for this work was provided by NIH grants NIH RO1 NS092870 and NIH U54 HD090256
Support was also provided by the Science and Medicine Scholars Graduate Research Fellowship Program.
This material is also based upon work supported by the National Science Foundation Graduate Research Fellowship Program under Grant No.DGE-1747503. Any opinions, findings, and conclusions or recommendations expressed in this material are those of the author(s) and do not necessarily reflect the views of the National Science Foundation.
References
1. Hillary FG, Slocomb J, Hills EC, et al. Changes in resting connectivity during recovery from severetraumatic brain injury. International journal of psychophysiology : official journal of the InternationalOrganization of Psychophysiology 2011;82:115-23.
2. Anderson V, Catroppa C. Memory outcome at 5 years post-childhood traumatic brain injury. Brain injury : [BI] 2007;21:1399-409.
3. Fay TB, Yeates KO, Wade SL, Drotar D, Stancin T, Taylor HG. Predicting longitudinal patterns of functional deficits in children with traumatic brain injury. Neuropsychology 2009;23:271-82.
4. Varentsova A, Zhang S, Arfanakis K. Development of a high angular resolution diffusion imaging human brain template. Neuroimage 2014;91:177-186.
5. Avants B.B. et al. (2012) A Unified Image Registration Framework for ITK. In: Dawant B.M., Christensen G.E., Fitzpatrick J.M., Rueckert D. (eds) Biomedical Image Registration. WBIR 2012. Lecture Notes in Computer Science, vol 7359. Springer, Berlin, Heidelberg
6. Beers SR, Wisniewski SR, Garcia-Filion P, et al. Validity of a pediatric version of the Glasgow OutcomeScale-Extended. Journal of neurotrauma 2012;29:1126-39.
7. McCauley SR, Wilde EA, Anderson VA, et al. Recommendations for the use of common outcomemeasures in pediatric traumatic brain injury research. Journal of neurotrauma 2012;29:678-705.
8. Gioia G, Isquith P, Hoffhines V, Guy S. Behavior Rating Inventory of Executive Function. PyschologicalAssessment Resources 2000;Odessa, FL.
9. Kurowski BG, Wade SL, Kirkwood MW, et al. Association of parent ratings of executive function withglobal- and setting-specific behavioral impairment after adolescent traumatic brain injury. Archives of physical medicine and rehabilitation 2013;94:543-50.
10. Delis D, Kramer JH, Kaplan E, Ober B. California Verbal Learning Test - Children's Version. Psychological Corporation;San Antonio, TX.
11. Marquez de la Plata CD, Garces J, Shokri Kojori E, et al. Deficits in functional connectivity ofhippocampal and frontal lobe circuits after traumatic axonal injury. Archives of neurology 2011;68:74-84.
12. Ewing-Cobbs L, Prasad MR, Swank P, et al. Arrested development and disrupted callosal microstructurefollowing pediatric traumatic brain injury: relation to neurobehavioral outcomes. NeuroImage2008;42:1305-15.
13. Wilde EA, Ramos MA, Yallampalli R, et al. Diffusion tensor imaging of the cingulum bundle in children after traumatic brain injury. Developmental neuropsychology 2010;35:333-51.
14. Bendlin BB, Ries ML, Lazar M, et al. Longitudinal changes in patients with traumatic brain injury assessed with diffusion-tensor and volumetric imaging. NeuroImage 2008;42:503-14.
Figures