3009
Altered Functional Connectivity during N-Back Task is Associated with Cognitive Deficits in Mild Traumatic Brain Injury1Translational Imaging Research Center, Taipei Medical University Hospital, Taipei, Taiwan, 2Department of Radiology, School of Medicine, College of Medicine, Taipei Medical University, Taipei, Taiwan, 3Department of Biomedical Imaging and Radiological Sciences, National Yang-Ming University, Taipei, Taiwan, 4Department of Medical Imaging, Taipei Medical University Hospital, Taipei, Taiwan
Synopsis
A subgroup of patients with mild traumatic brain injury (mTBI) suffers from a series of cognitive symptoms, including the memory loss and attention deficit. In our study, we investigated the alterations of functional connectivity during N-back working memory task in 46 mTBI and 43 HC using independent component analysis. Despite both groups revealed comparable performances during task, mTBI showed lower functional connectivity in several task-related neural networks that can be correlated with the cognitive complaints. We concluded that the alterations of neural networks may indicate cognitive symptoms after mTBI.
Introduction
Cognitive deficits, such as attention deficiency, memory loss, and executive function abnormality, are constantly reported in patients with mild traumatic brain injury (mTBI)1. However, the neural correlates still remain unclear2. In this study, we aim to investigate the association between severity of cognitive deficits and functional connectivity during working memory task using fMRI.Methods
Participants: We included 46 mTBI patients, who fulfilled the diagnosis criteria of American Congress of Rehabilitation Medicine3, and 43 healthy controls (HC). All patients were assessed within 1 month after injury. Each participant signed informed consent forms approved by Taipei Medical University Joint Institutional Review Board.
Psychological assessment: Before the acquisition of MRI data, participants performed Rivermead Post Concussion Symptoms Questionnaire (PCSQ), including cognitive, emotion, and somatic sub-domains4. Participants’ cognitive functions were assessed using Wechsler Adult Intelligence Scale (WAIS)-IV. Working memory index (WMI) and processing speed index (PSI) were calculated to represent the memory and executive control abilities5.
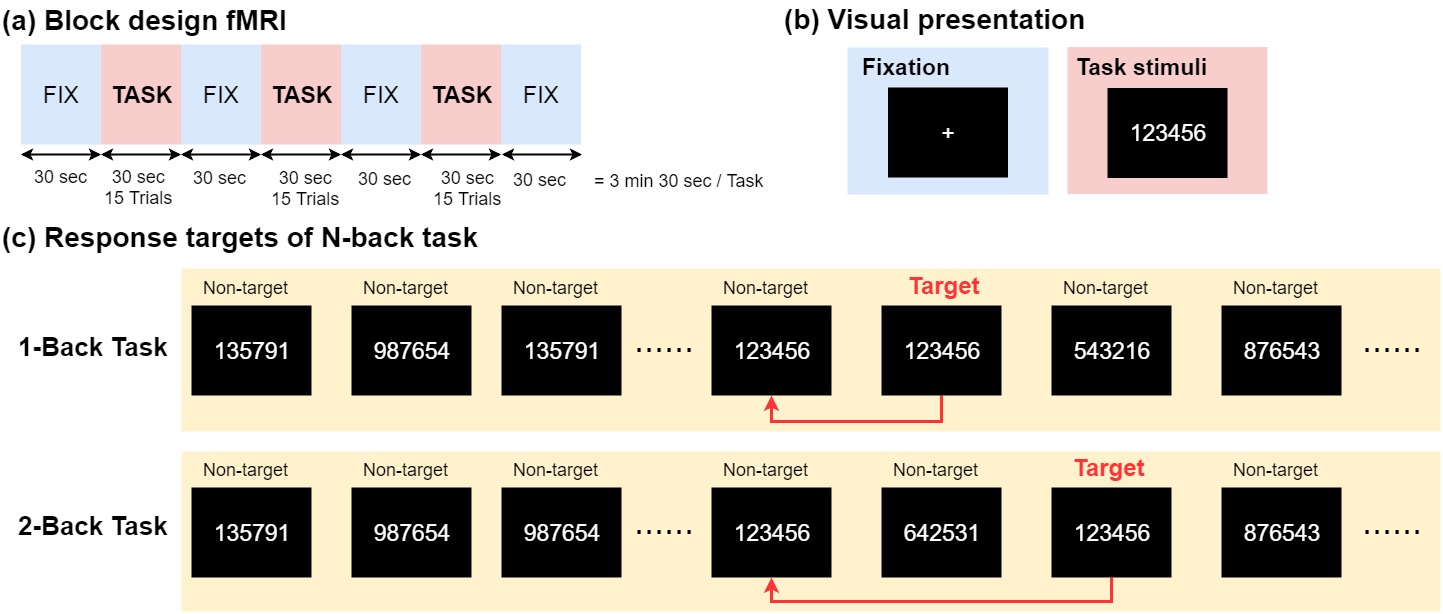
Working Memory Task: The experimental design of N-back task in fMRI is depicted in Fig. 1 and was performed using Presentation software (Version 18.1, Neurobehavioral Systems, Inc., Berkeley, CA). During n-back tasks, participants were told to respond whenever the current stimulus matched the number that had been presented n back previously (n = 1 or 2).
MR acquisition: Images were acquired on a 3T MRI scanner (MAGNETOM Prisma, Siemens) using a 20-channel head coil. Structural 3D T1-weighted images were acquired using magnetization-prepared rapid acquisition with gradient echo (MPRAGE) sequence, with the following parameters: repetition time (TR)=2300ms, echo time (TE)=3.3ms, flip angle (FA)=8˚, 176 axial slices, field of view (FOV)=256×256×176mm3, voxel size=1x1x1mm3. During fMRI sessions, 105 echo-planar imaging scans were acquired for 1-back task and 2-back task using the following parameters: TR=2000ms, TE=20ms, FA=90˚, 40 axial slices with slice thickness=3.5mm, FOV=210×210mm2, voxel size=3.0x3.0x3.5mm3.
Preprocessing: The standard preprocessing steps were conducted using SPM12 software (Wellcome Trust Centre for Neuroimaging, London, UK; http://www.fil.ion.ucl.ac.uk) which was implemented within MATLAB R2016b (The MathWorks, Inc., Natick, Massachusets, USA), including slice timing correction, realignment, co-registration, normalization to MNI space, and spatial smoothing using 6-mm FWHM Gaussian kernel. Participants with excessive head motion had been excluded from the subsequent analyses.
Independent component analysis (ICA): The group ICA were performed on preprocessed fMRI data of 89 participants using GIFT software version 3.0b (http://mialab.mrn.org/software/gift/). First, the optimal number of independent components (ICs) were estimated to be 20 using the minimum description length criteria6. The functional data were decomposed into 20 ICs with the infomax algorithm7. The most stable estimation of ICs was obtained by re-running ICA for 100 times using the ICASSO method8. Finally, single subject time courses and spatial maps were back-reconstructed. The spatial maps of ICs during 1-back and 2-back tasks for each subject were z-transformed to obtain ICA z-maps.
Statistics: An one-sample T test on each ICA z-map across subjects was performed to create binary component masks followed by a two-sample T test to investigate the group differences of each ICA z-map within the component masks. Six-mm radius spheres around regions with group difference were applied to calculate the averaged z-values. Finally, partial correlation analyses between behavioral measures related to cognitive deficits and averaged z-values were performed, controlling for age and sex.
Results
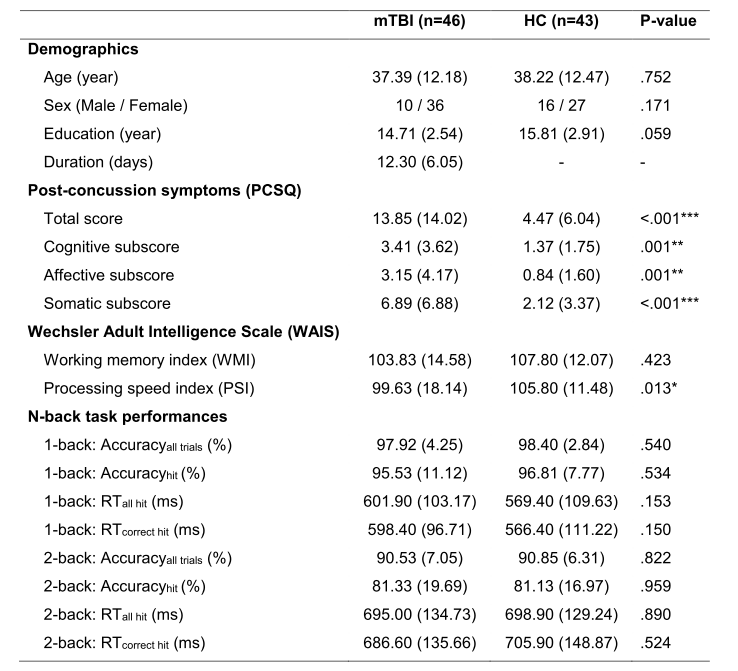
Behaviors: Demographics, PCSQ, WAIS, and N-back task performances are presented in Table 1. Compared to HC, mTBI showed higher PCSQ total score and subscores, and lower PSI. However, both groups showed no difference in performances during N-back task.
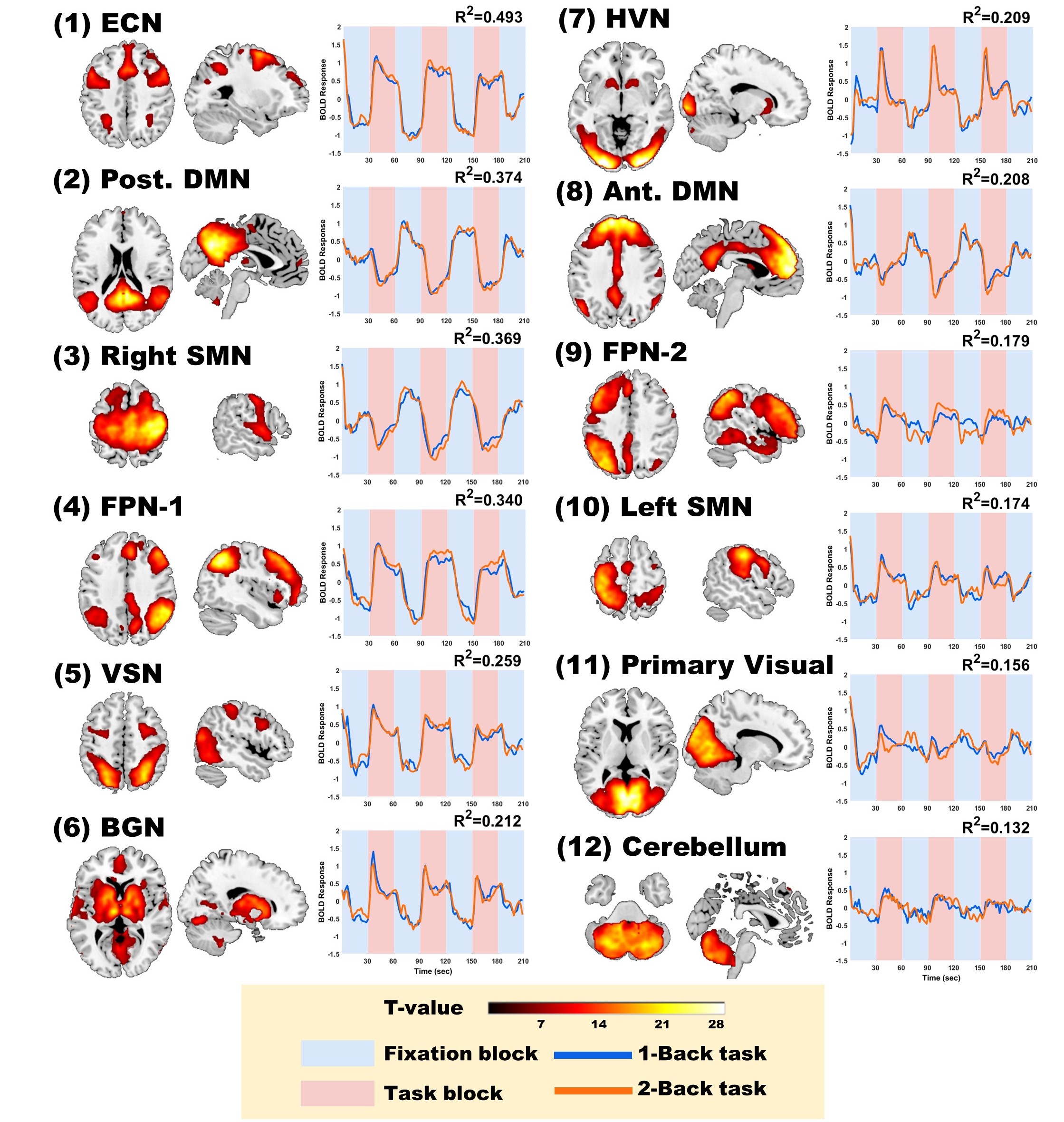
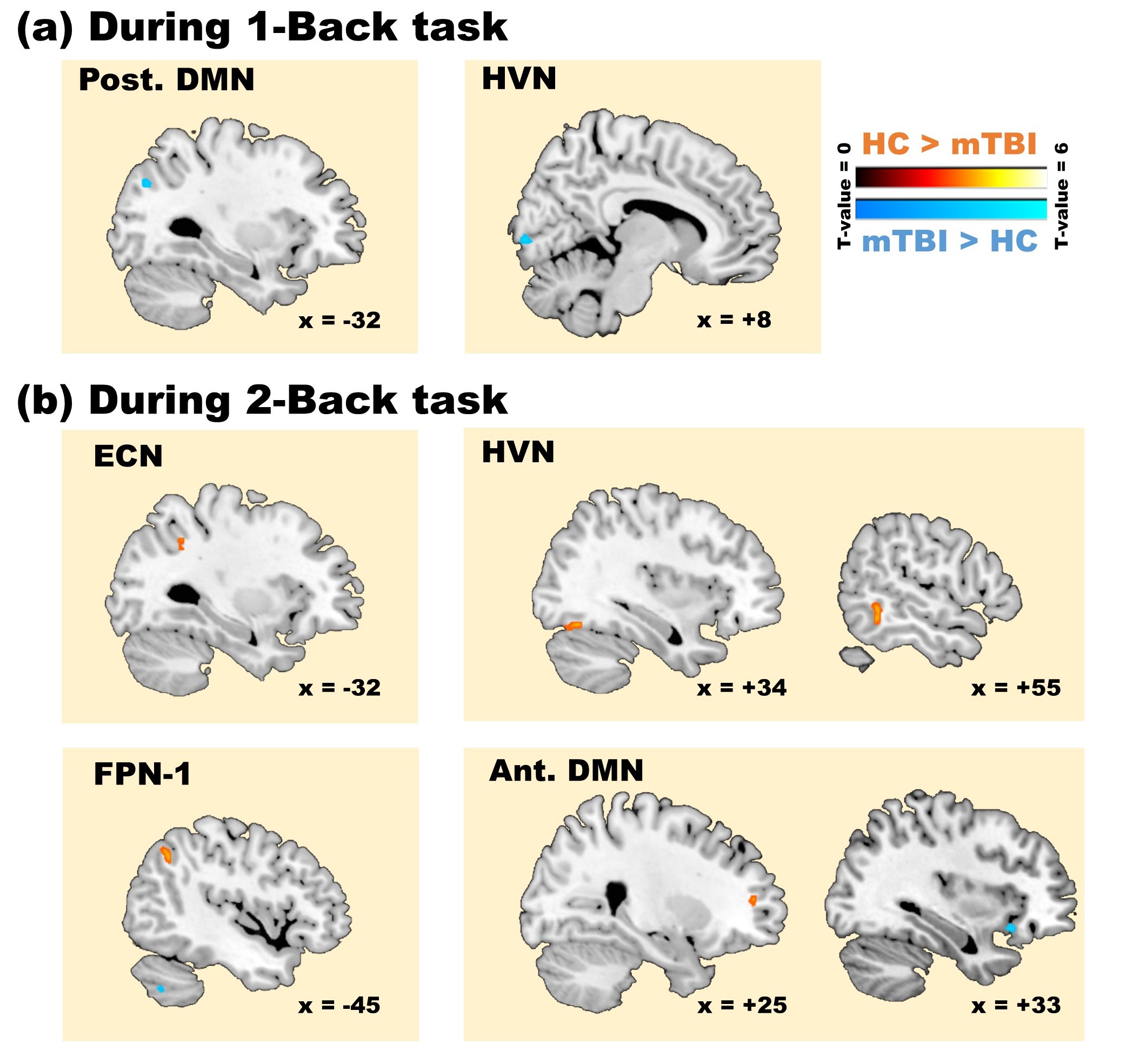
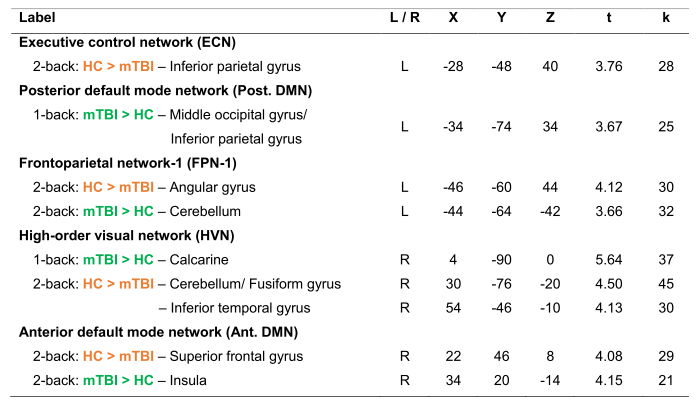
Functional connectivity (FC): The spatial patterns of 12 task-related ICs were shown in Figure 2. Among them, 5 ICs showed significant differences between mTBI and HC (Fig. 3; Table 2). During 1-back task, mTBI showed higher FC in the Post. DMN and HVN. On the other hand, during 2-back task, mTBI mostly showed lower FC, for example, in ECN and HVN.
Behaviors-ICs relationships: Partial correlation results showed that the cognitive subscore of PCSQ is negatively correlated with FCs of inferior parietal gyrus in ECN (partial r=-0.222, p=0.039), angular gyrus in FPN-1 (partial r=-0.245, p=0.022), and superior frontal gyrus in Ant. DMN (partial r=-0.237, r=0.027) during 2-back task.
Discussion
In this study, the extents of cognitive deficits after mTBI were correlated to the alterations of several functional networks, such as ECN, FPN, and Ant. DMN, during 2-back task. These results indicate that the abnormal FCs associated with frontal and parietal regions, and the degradation of DMN deactivation during task at high-cognitive load might be potential image biomarkers for probing cognitive complaint in patients with mTBI.Acknowledgements
Our work was supported by grants MOST104-2923-B-038-003-MY3 and MOST106-2314-B-010-058-MY2 from the Ministry of Science and Technology of Taiwan.References
1. Belanger H, Curtiss G, Demery J, et al. Factors moderating neuropsychological outcomes following mild traumatic brain injury: a meta-analysis. J Int Neuropsychol Soc. 2005;11(3):215-227.
2. Sharp D, Scott G, & Leech R. Network dysfunction after traumatic brain injury. Nat Rev Neurol. 2014;10(3):156-166.
3. Definition of mild traumatic brain injury. Journal of Head Trauma Rehabilitation. 1993;8(3):86-87.
4. Potter S, Leigh E, Wade D, et al. The Rivermead post concussion symptoms questionnaire. J Neurol. 2006;253(12):1603-1614.
5. Carlozzi E, Kirsch L, Kisala A, et al. An examination of the Wechsler Adult Intelligence Scales, (WAIS-IV) in individuals with complicated mild, moderate and Severe traumatic brain injury (TBI). The Clinical Neuropsychologist. 2015;29(1):21-37.
6. Li Y, Adalı T., & Calhoun V. Estimating the number of independent components for functional magnetic resonance imaging data. Hum Brain Mapp. 2007;28(11):1251-1266.
7. Bell J & Sejnowski J. An information maximisation approach to blind separation and blind deconvolution. Neural Comput. 1995;7(6):1129-1159.
8. J. Himberg & A. Hyvärinen. Icasso: software for investigating the reliability of ICA estimates by clustering and visualization. In Proc. 2003 IEEE Workshop on Neural Networks for Signal Processing (NNSP2003). Toulouse, France, 2003, September. pp. 259-268.
Figures