3004
Changes in Cerebral Blood Flow after Youth Sport-Related Concussion and with Recovery1Biomedical Engineering Graduate Program, University of Calgary, Calgary, AB, Canada, 2Faculty of Kinesiology and Departments of Pediatrics and Community Health Sciences, University of Calgary, Calgary, AB, Canada, 3Department of Clinical Neurosciences, University of Calgary, Calgary, AB, Canada, 4Dept of Radiology, University of Calgary, Calgary, AB, Canada
Synopsis
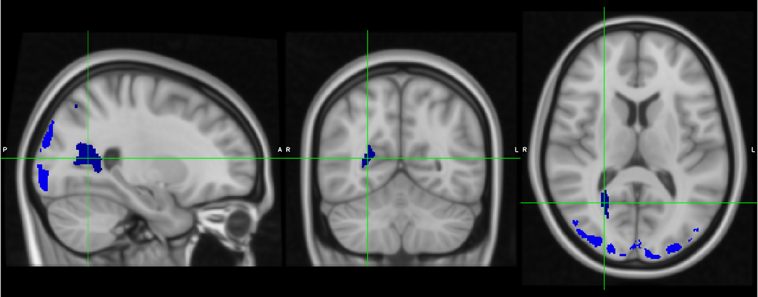
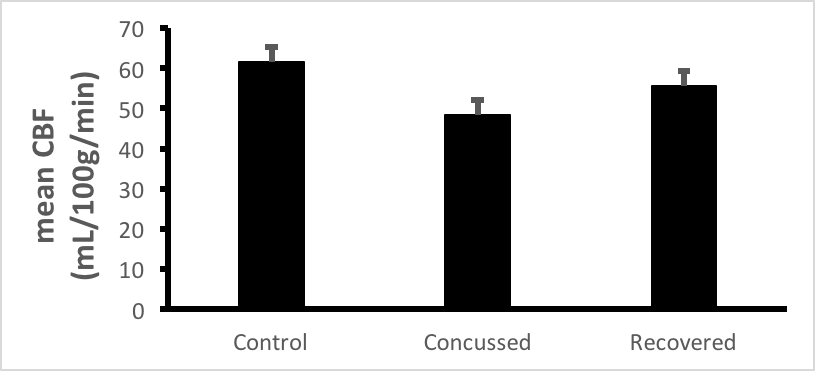
Mild traumatic brain injury (mTBI), including sport-related concussion, is a major health issue. Changes in cerebral blood flow (CBF) following concussion, as measured by arterial spin labeling (ASL) MRI, may potentially be an indicator of injury or recovery. Compared to healthy controls, we found that CBF was significantly decreased in recently concussed youth ( within 14 days post-injury) within the regions of the occipital and parietal lobes, including the right precuneus. For these regions, CBF of recovered youth was greater than recently concussed and less than controls, though not significantly different from either group.
Introduction
Mild traumatic brain injury (mTBI), including sport-related concussion, has become a major health issue. By the age of 25, the lifetime prevalence of a TBI may be as high as 30%, and as much as 90% of cases are of mild severity [1]. In the case of severe TBI, an acute decrease in cerebral blood flow (CBF) (hypoperfusion) occurs on the first day, then increased CBF (hyperemia) occurs and lasts for 1 to 3 days, followed by another decrease in CBF that lasts from a few days to a few weeks [2,3,4]. The time course of changes in CBF over time following mild TBI are not understood, nor its relationship to cerebral metabolic rate, vascular reactivity and outcome [4,5]. Using arterial spin labeling (ASL) MRI, previous studies have reported both increases and decreases in CBF after mTBI, and studies have varied in time of imaging post-injury, symptom severity, as well as brain region of interests (ROIs) under examination [4,6,7,8]. In the current study, we used ASL to quantify CBF in three groups of youth hockey players: players recently concussed and symptomatic, players recovered from concussion and were cleared to play, and healthy controls.Method
Seventy six youth hockey players (30 recently concussed, 21 recovered, and 25 healthy controls with no history of concussion; age range 11-18 years; 61 male and 15 female) were recruited. Recently concussed subjects underwent MRI within 14 days of injury (average 7.3 ±3.3 days between concussion and scanning for recently concussed subjects), and recovered subjects underwent MRI within 7 days of being cleared to return to play (36.57 ±16.57 days between concussion and scanning for recovered subjects). ASL was performed using 3 Tesla GE Discovery MR750w (GE Healthcare ,Waukesha, WI) scanners at Alberta Children’s hospital (13 recently concussed, 21 recovered and 15 controls) and Seaman Family MR Research Centre (17 recently concussed, 10 controls) with 3.5-mm slice thickness. Quantitative Cerebral Blood Flow (CBF) maps were automatically calculated from the 3D ASL scan using the GE scanner-integrated pipeline with default settings. Two step co-registration was performed to transform the raw ASL images into MNI space using corresponding T1-weighted images. These transformation matrices were then used to bring the CBF maps into MNI space.
A whole brain gray matter voxel-by-voxel analysis was performed among the three groups, using FSL’s general linear model (GLM) approach with the randomise option to correct for multiple comparisons. The MNI tissue probability map was thresholded at gray matter probability >25% to create a gray-matter mask in order to constrain the statistical comparisons to gray matter only. Demeaned age, sex and scanner site were used as covariates in the GLM model to remove any effect from these factors.
Results and Discussion
The recently concussed group exhibited significantly reduced CBF, compared to healthy controls, in parts of occipital and parietal lobes, including the right precuneus (Figure 1). No statistically significant group difference was found between recovered and control groups nor between recovered and recently concussed groups, for whole brain voxel-by-voxel analysis. Upon direct examination of the ROIs in the recently concussed vs. control map, mean CBF of the recovered group was in between that of the recently concussed and control groups, though not significantly different from either group.Conclusions
CBF following sport-related concussion is redcued in posterior regions of the brain, which seems to normalize with recovery. These results demonstrate the potential of ASL as both an indicator of injury and recovery. The lack of statistical significance between the recovered group and the other groups may be the result of low patient numbers. Future longitudinal studies at different time points while subjects are still symptomatic will help establish the utility of ASL in the assessment of mTBI. Acknowledgements
We acknowledge the support of the Canadian Institutes of Health Research, Alberta Innovates Health Solutions, the Alberta Children’s Hospital Foundation (Vi Riddell Pediatric Rehabiltation Research Program, Integrated Concussion Research Program), Winsport and NSERC CREATE i3t Program. The Sport Injury Prevention Research Centres is one of ten International Olympic Committee Research Centres for Injury and Illness Prevention and Protection of the Athlete. Thank you to the players, parents, coaches, and Hockey Calgary for your support and shared vision in evidence-informed prevention and management of concussions in youth ice hockey players.References
1. McKinlay, A et al. Prevalence of traumatic brain injury among children, adolescents and young adults: prospective evidence from a birth cohort. Brain Inj. 22, 175 -181 (2008).
2. Adelson, P.D., Srinivas, R., Chang, Y., Bell, M., and Kochanek, P.M. Cerebrovascular response in children following severe traumatic brain injury. Childs Nerv. Syst. 27, 1465–1476 (2011).
3. Martin, N.A., Patwardhan, R.V., Alexander, M.J., Africk, C.Z., Lee, J.H., Shalmon, E., Hovda, D.A., and Becker, D.P. Char- acterization of cerebral hemodynamic phases following severe head trauma: hypoperfusion, hyperemia, and vasospasm. J. Neurosurg. 87, 9–19 (1997).
4. Karen M. Barlow, Lorenzo D. Marcil, Deborah Dewey, Helen L. Carlson, Frank P. MacMaster, Brian L. Brooks, and R. Marc Lebel. Cerebral Perfusion changes in Post-Concussion Syndrome: A prospective controlled cohort study. J. Neurotrauma 33:1–9 (2016).
5. Len, T.K., and Neary, J.P. Cerebrovascular pathophysiology following mild traumatic brain injury. Clin. Physiol. Funct. Imaging 31, 85–93 (2011).
6. Lin C-M, Tseng Y-C, Hsu H-L, Chen C-J, Chen DY-T, Yan F-X, et al. Arterial Spin Labeling Perfusion Study in the Patients with Subacute Mild Traumatic Brain Injury. PLoS ONE 11(2): e0149109. doi:10.1371/journal.pone.0149109 (2016)
7. A., Stephens Jaclyn ; Peiying, Liu ; Hanzhang, Lu ; J., Suskauer Stacy. Cerebral Blood Flow after Mild Traumatic Brain Injury: Associations between Symptoms and Post-Injury Perfusion. J. Neurotrauma, Vol.35(2), p.241(8) ( 2018)
8. Wang, Y., West, J.D., Bailey, J.N., Westfall, D.R., Xiao, H., Arnold, T.W., Kersey, P.A., Saykin, A.J., and McDonald, B.C. De- creased cerebral blood flow in chronic pediatric mild TBI: an MRI perfusion study. Dev. Neuropsychol. 40, 40–44 (2015).
Figures