2994
The relationship between baseline PETCO2 measurements and cerebral blood flow: The importance of resting vascular tension in perfusion-based studies1Queen's University, Kingston, ON, Canada
Synopsis
Measures of cerebral blood flow (CBF) are often used to examine cerebral physiology after sport-related concussion. Carbon dioxide modulates CBF and determines resting vascular tension yet studies rarely account for this. This study examined the effect of the end tidal partial pressure of carbon dioxide (PETCO2) on CBF in athletes. PETCO2 accounted for 14% of the variance in CBF and this increased to 37% when age and sex were included. No prior studies examining SRC and CBF have accounted for resting PETCO2. Future studies should move from univariate to multivariate methods to ensure that CBF-based estimates are interpreted correctly.
Introduction
In recent years, the acute and chronic effects of concussive and repetitive subconcussive head impacts on brain structure and function have received increasing attention.1–4 In particular, alterations in cerebral blood flow (CBF) acutely after concussion have been demonstrated.5–7 The partial pressures of arterial gases, and especially carbon dioxide (CO2), are an important modulator of CBF,8 and thus, influence the resting tone of the vasculature. As well, the magnitude of change in CBF for a change in the partial pressure of carbon dioxide, known as cerebrovascular reactivity, is affected by basal vascular tension. Despite this knowledge that the partial pressure of CO2, typically measured as the end tidal partial pressure of CO2 (PETCO2) affects CBF, the magnitude of this affect is unknown. Therefore, the purpose of this study was to determine the strength of the relationship between resting vascular tension, quantified as PETCO2, and CBF in a cohort of healthy athletes to review whether previous concussion studies account for this relationship.Methods
This study included a cohort of 64 athletes (20 ± 3 years, 15 females) with no history of concussion. Subjects completed a six-minute boxcar hypercapnia protocol (Figure 1), with PETCO2 and PETO2 targeted using a feed-forward computerized gas delivery system (RespirActTM, Thornhill Research Inc., Toronto, ON). Perfusion data was acquired using a dual echo pseudo-continuous ASL sequence with the following parameters: TR = 4000 ms, TE1/TE2 = 10/30 ms, FOV = 250 x 250 mm, flip angle = 90°, voxel size = 3.9 mm isotropic, post-labeling delay (PLD) = 1000 ms, slice gap = 0.773 mm, label offset = 100 mm, receiver bandwidth = 2604 Hz/pixel, EPI factor = 64, tagging duration 1.665s.9 A tissue magnetization map (M0) with no spin labelling and a longer TR (15 000 ms) was also acquired for estimation of CBF. Perfusion-weighted images were extracted from the first echo (TE = 10 ms) using a linear surround subtraction between the control and tag images,10 and converted into physiological units (mL/100g/min) using the single-blood compartment model.11 Mean baseline grey-matter (CBF0) was determined from the 120s baseline period after removal of the first 20s to allow PETCO2 to stabilize. A linear regression was performed with CBF0 as the dependent variable with age, PETCO2, and sex included in the model (SPSS Inc., Chicago, IL, USA).
Results and Discussion
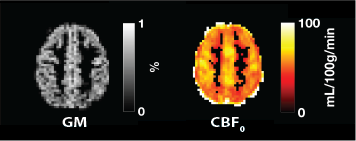
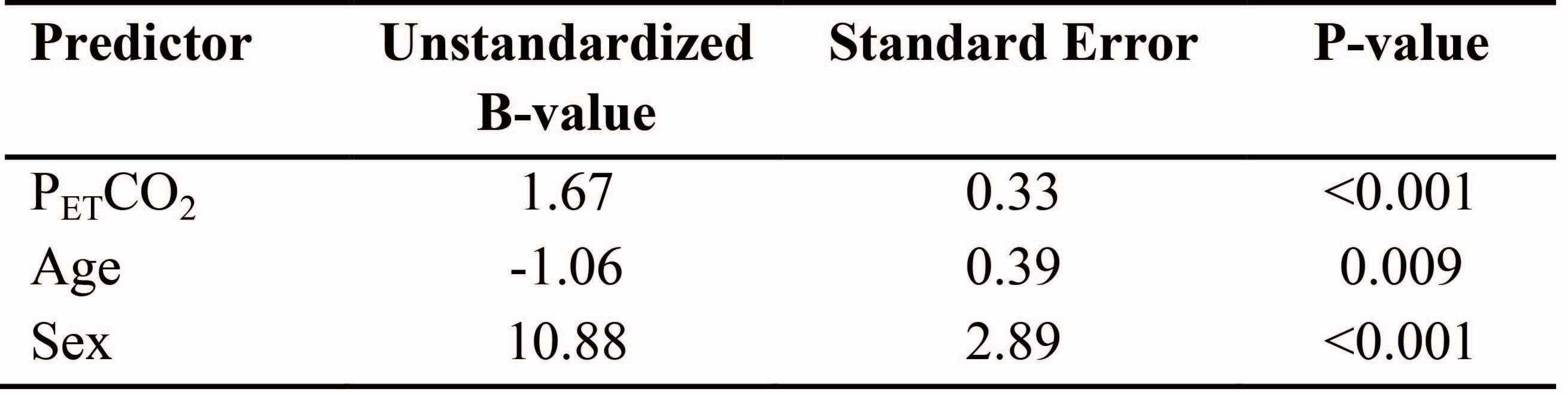
Mean CBF0 was 64 ± 10 ml/100g/min while the average PETCO2 for the group was 40 ± 4 mmHg. Representative maps are shown in Figure 2. There was a significant relationship between resting PETCO2 and CBF0 (Figure 3). Additionally, when entered into a regression model, age, sex, and PETCO2 were significant predictors of CBF0 (Table 1) and these three variables accounted for 37% of the variance in CBF. Despite the fact that all three variables examined in this study were significant predictors of CBF, the analyses often employed, particularly in the concussion literature (Table 2), examines CBF0 in a univariate fashion by comparing between groups or time points.5,6,12–14 This study indicates that resting vascular tension, is an important regulator of CBF0 and should be included as a covariate in all analyses that attempt to draw conclusions about cerebral hemodynamics.Acknowledgements
No acknowledgement found.References
References
1. McCrea, M. et al. Acute effects and recovery time following concussion in collegiate football players: the NCAA Concussion Study. Jama 290, 2556–2563 (2003).
2. Guskiewicz, K. M. et al. Recurrent concussion and risk of depression in retired professional football players. Med. Sci. Sports Exerc. 39, 903–909 (2007).
3. Guskiewicz, K. M. et al. Cumulative effects associated with recurrent concussion in collegiate football players: the NCAA Concussion Study. JAMA 290, 2549–55 (2003).
4. Slobounov, S. M. et al. The effect of repetitive subconcussive collisions on brain integrity in collegiate football players over a single football season: a multi-modal neuroimaging study. NeuroImage Clin. 14, 708–718 (2017).
5. Wang, Y. et al. Cerebral blood flow in acute concussion: preliminary ASL findings from the NCAA-DoD CARE consortium. Brain Imaging and Behavior (2018). doi:10.1007/s11682-018-9946-5
6. Barlow, K. M. et al. Cerebral perfusion changes in post-concussion syndrome: a prospective controlled cohort study. J. Neurotrauma 33, 1–9 (2016).
7. Meier, T. B. et al. Recovery of cerebral blood flow following sports-related concussion. JAMA Neurol. 87106, 1–9 (2015).
8. Willie, C. K. et al. Regional brain blood flow in man during acute changes in arterial blood gases. J. Physiol. 590, 3261–3275 (2012).
9. Wu, W., Buxton, R. B. & Wong, E. C. Vascular space occupancy weighted imaging with control of residual blood signal and higher contrast-to-noise ratio. IEEE Trans. Med. Imaging 26, 1319–27 (2007). 10. Germuska, M. et al. A forward modelling approach for the estimation of oxygen extraction fraction by calibrated fMRI. Neuroimage 139, 313–323 (2016).
11. Wang, J. et al. Arterial transit time imaging with flow encoding arterial spin tagging (FEAST). Magn. Reson. Med. 50, 599–607 (2003).
12. Mutch, W. A. C. et al. Brain magnetic resonance imaging CO2 stress testing in adolescent postconcussion syndrome. J. Neurosurg. 125, 648–660 (2016).
13. Mutch, W. A. C. et al. Longitudinal brain magnetic resonance imaging CO2 stress testing in individual adolescent sports-related concussion patients: A pilot study. Front. Neurol. 7, 1–8 (2016).
14. Churchill, N. W. et al. The first week after concussion: Blood flow, brain function and white matter microstructure. NeuroImage Clin. 14, 480–489 (2017).
15. Wang, Y. et al. Cerebral blood flow alterations in acute sport-related concussion. J. Neurotrauma 33, 1227–1236 (2016).
16. Stephens, J. A., Liu, P., Lu, H. & Suskauer, S. J. Cerebral Blood Flow after Mild Traumatic Brain Injury: Associations between Symptoms and Post-Injury Perfusion. J. Neurotrauma neu.2017.5237 (2017). doi:10.1089/neu.2017.5237
17. Churchill, N. W., Hutchison, M. G., Graham, S. J. & Schweizer, T. A. Symptom correlates of cerebral blood flow following acute concussion. NeuroImage Clin. 16, 234–239 (2017).
18. Mutch, W. A. C. et al. Patient-specific alterations in CO2 cerebrovascular responsiveness in acute and sub-acute sports-related concussion. Front. Neurol. 9, (2018).
19. Maugans, T. A., Farley, C., Altaye, M., Leach, J. & Cecil, K. M. Pediatric sports-related concussion produces cerebral blood flow alterations. Pediatrics 129, 28–37 (2012).
Figures