2992
The clinical condition to be assessed by radiological assessment significantly influences the radiological scores of Compressed Sensing accelerated 3D brain MRI1Institute for Digital Communications, University of Edinburgh, Edinburgh, United Kingdom, 2Centre for Clinical Brain Sciences, University of Edinburgh, Edinburgh, United Kingdom
Synopsis
This study shows that it is important to clearly define the correct clinical question that needs to be answered before the radiological assessment of accelerated 3D gradient echo brain scans for clinical diagnosis.
Purpose
The main purpose of this study was to investigate whether radiological scores (RS) are influenced by the clinical question being asked by radiologists during assessment of fully sampled (FS) and accelerated 3D brain scans. It has already been shown that in certain clinical sequences, the k-space acquisition order is essential for obtaining the optimal contrast in FS and subsampled compressed sensing (CS) acquisitions1. It has also been shown that CS accelerated prospective 3D brain scans can be clinically useful for diagnosis in some cases2. In this study, we show that the diagnostic utility of CS accelerated prospective 3D brain scans is highly dependent on the clinical question being answered by radiological assessment.Methods
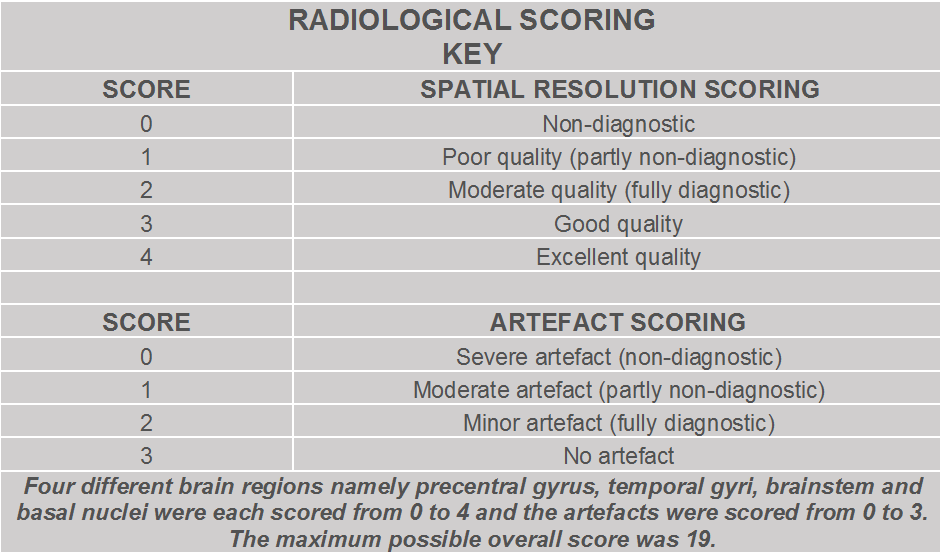
The scanning was performed on a 1.5T GE Signa Horizon HDX scanner on 8 healthy volunteers after informed consent was obtained. The manufacturer’s Inversion Recovery prepared 3D Gradient Echo (GRE) sequence was used to collect FS and accelerated subsampled brain datasets (using 3 different subsampling patterns with varying acceleration factors - R) whose k-space acquisition order was optimized for preserving optimal contrast2. Other sequence parameters were TR/TE/TI=10/4/500 ms; flip angle = 8°; matrix 192×192×160 slices; isotropic 1.3 mm voxels and the images were reconstructed using the CS and parallel imaging based NESTA algorithm3. The scan time was reduced from 8:08 minutes to 2:42 minutes for R=3. The acquired datasets were then randomized and given to two neuroradiologists with more than ten years experience for blinded assessment of image quality and artefacts using a common radiological scoring key from the literature4. The scoring key is shown in Table 1 with ‘0’ being non-diagnostic and ‘4’ being excellent quality for four different brain regions while the artefacts were scored with ‘0’ meaning severe artefact and ‘3’ meaning no artefact2,4.Results
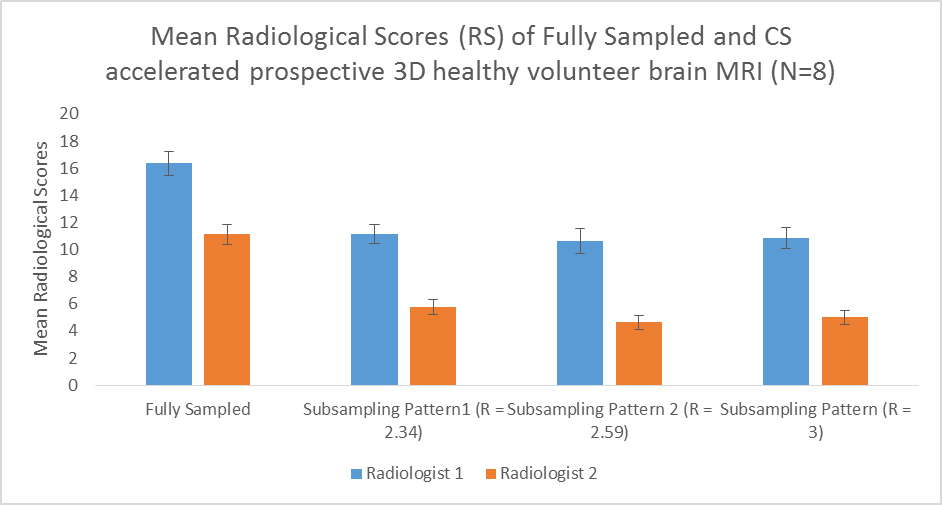
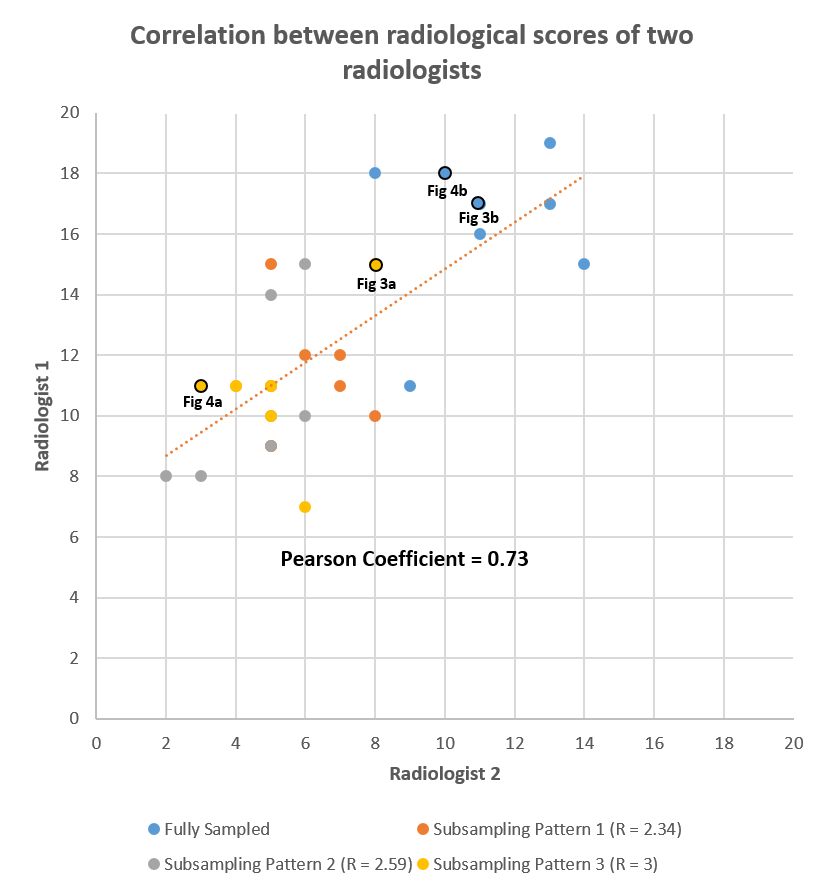
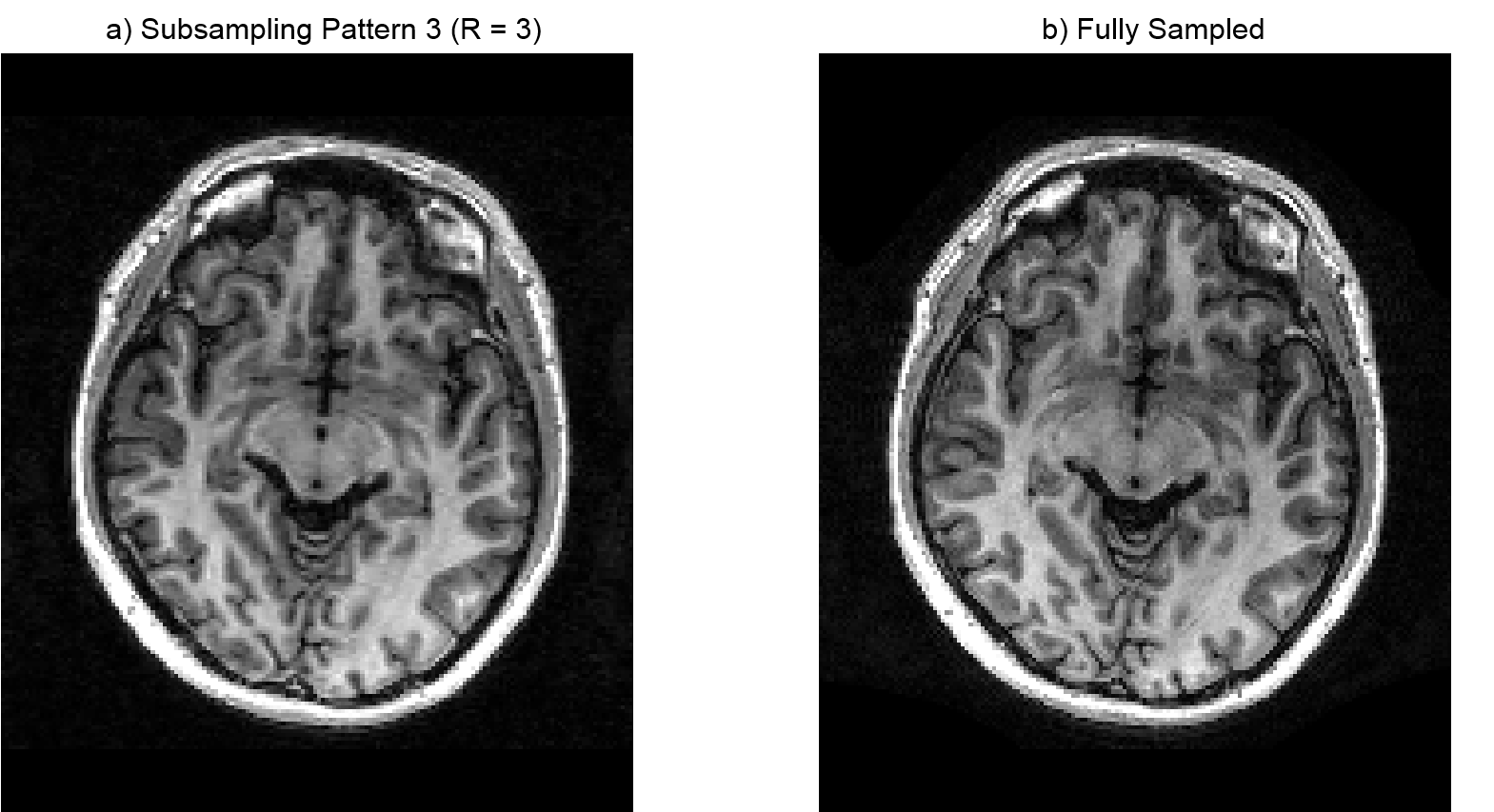
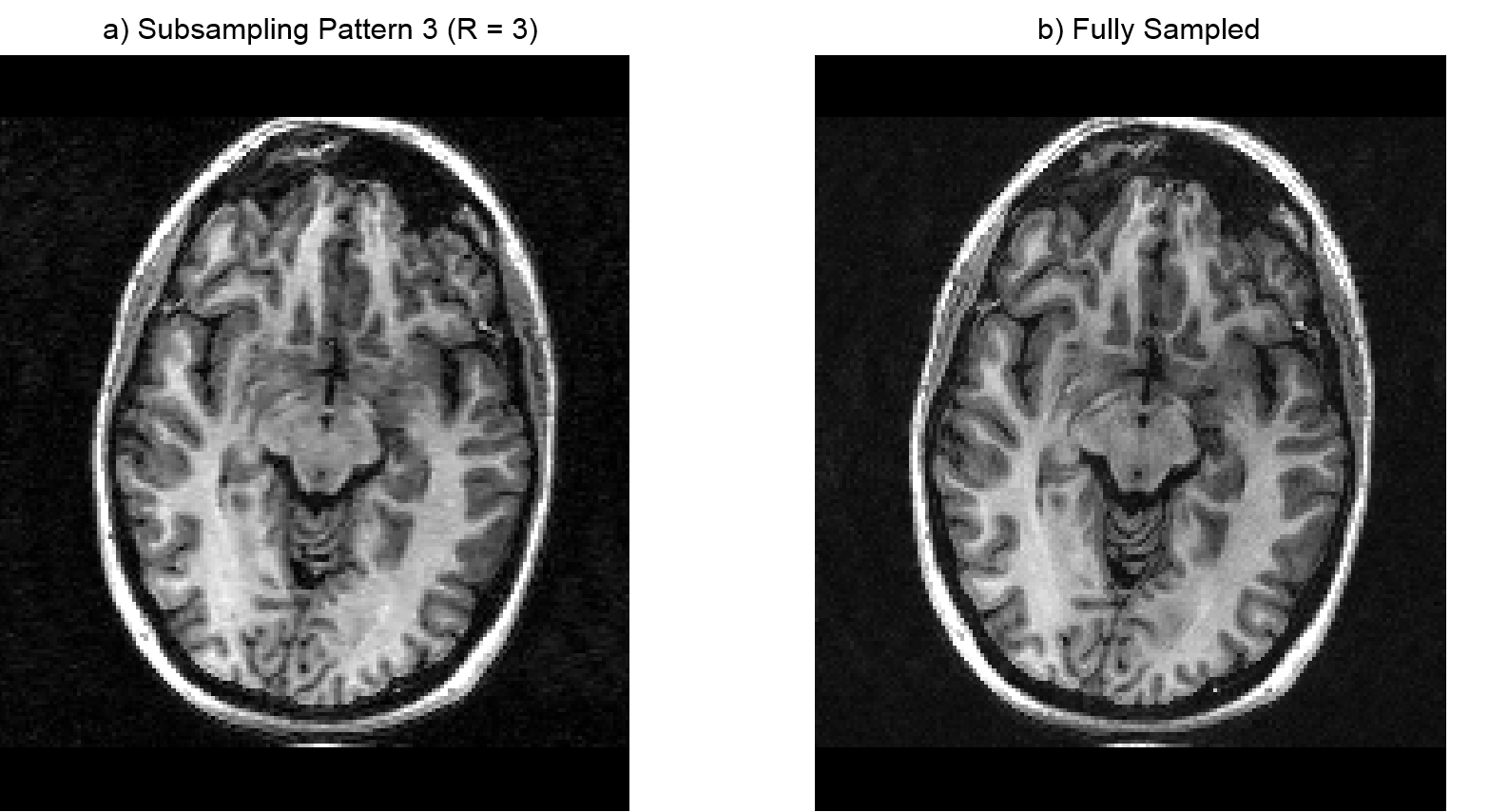
Fig. 1 shows the overall mean RS along with standard error (SE) of both neuroradiologists for FS and three different sampling order optimized accelerated datasets with varying acceleration factors. Fig. 2 shows the correlation of RS between the two neuroradiologists for all the datasets (8 subjects x 4 datasets = 32 datasets). Fig. 3a shows a CS reconstructed image slice that was found to be clinically suitable for gross structural assessment of the brain, e.g. identifying space occupying lesions such as tumours. Fig. 4a shows a CS reconstructed image slice that was considered clinically not suitable for tasks that require high spatial resolution and grey-white matter differentiation, e.g. seeking developmental lesions responsible for epilepsy.Discussion and Conclusion
The scoring patterns of both radiologists were similar (see Fig. 1). In general, the FS datasets had higher scores compared to the CS accelerated scans. The correlation between the radiologists for different datasets was high (Pearson Coefficient = 0.73) which suggests that the two radiologists had a fairly strong degree of agreement between each other (see Fig. 2). Although both radiologists used the same scoring key, the amount of penalization that was applied to the RS varied because each radiologist was assessing the datasets based on a different theoretical clinical scenario. Radiologist 1 performed a routine structural assessment as might be applied in patients with non-specific headache and a clinical requirement to exclude tumour (based largely on grey and white matter boundaries, and cerebrospinal fluid distribution) and it was seen that CS accelerated scans were suitable in most cases leading to higher scores for image quality and artefacts (see Fig. 3). Radiologist 2 performed the assessment based on a practical clinical scenario for excluding lesions that might cause epilepsy (e.g. subtle developmental abnormalities of cortex, and measuring cortical thickness) and it was seen that the artefacts due to CS reconstruction were deemed to be more severe and impeded the clarity of certain brain structures like brainstem, cortical ribbon and basal ganglia (see Fig. 4), leading to lower scores for image quality and artefacts. Even though the radiologists assessed images based on different clinical questions, their overall mean RS followed a similar ranking pattern for both FS and CS accelerated scans as seen from Fig. 1; suggesting that the threshold used for radiological scoring strongly depended on the clinical condition to be assessed. Therefore, it is important to consider and clearly define the relevant clinical question before evaluating the diagnostic utility of CS accelerated prospective 3D brain scans. In conclusion, the selection of the degree of CS, as with other acceleration schemes, could be guided by the proposed clinical application, i.e. higher for standard clinical assessments, but reduced for usage scenarios where better tissue discrimination is needed as with epilepsy investigation.Acknowledgements
The research leading to these results has received funding from the European Union’s H2020 Framework Programme (H2020-MSCA-ITN-2014) under grant agreement no 642685 MacSeNet, the Engineering and Physical Sciences Research Council (EPSRC) platform grants, number EP/J015180/1 and EP/M019802/1.References
1. A. J. V. Benjamin, W. Bano, M. Davies, and I. Marshall, "Sampling Order Optimization for contrast preservation in accelerated prospective 3D MRI," in Proceedings of ESMRMB, #256, 2017.
2. A. J. V. Benjamin, W. Bano, G. Mair, M. Davies, and I. Marshall, "Sampling order optimization preserves contrast and improves clinical diagnostic utility of accelerated prospective 3D brain MRI: a radiological assessment study on healthy volunteers," in Proceedings of ISMRM, #3189, 2018.
3. S. Becker, J. Bobin, and E. J. Candès, "NESTA: A Fast and Accurate First-Order Method for Sparse Recovery," SIAM J. Img. Sci., vol. 4, pp. 1-39, 2011
4. S. Sirin, S. L. Goericke, B. M. Huening, A. Stein, S. Kinner, U. Felderhoff-Mueser, et al., "Evaluation of 100 brain examinations using a 3 Tesla MR-compatible incubator—safety, handling, and image quality," Neuroradiology, vol. 55, pp. 1241-1249, 2013.
Figures