2987
Fast multi-contrast EPI protocol: Preliminary experience with acute intracranial pathologies in the emergency department.Otto Rapalino1, Julian He1, Pamela Schaefer1, Matthew Christensen1, Arnaud Guidon2, Stefan Skare3, Tim Sprenger4, John Kirsch1, and Ramon Gilberto Gonzalez1
1Radiology, Massachusetts General Hospital, Boston, MA, United States, 2GE Healthcare, Boston, MA, United States, 3Karolinska Institute, Karolinska, Sweden, 4Karolinska Institute, Stockholm, Sweden
Synopsis
Prospective analysis of the diagnostic performance of a fast multi-contrast EPI sequence compared to conventional sequences. A sample of 30 cases (out of 190) was evaluated and head-to-head comparisons were performed for the visualization of clinically relevant intracranial pathologies. Our findings suggest that this multi-contrast EPI sequence could potentially provide an acceptable diagnostic alternative to the core conventional brain MRI sequences in selected populations that cannot tolerate long MRI examinations in the Emergency Department.
INTRODUCTION:
Acquisition times with MRI are usually significantly longer compared to CT and MRI sequences with long acquisition times are more susceptible to motion artifacts. Long MR acquisition times can present a significant challenge in some clinical populations (e.g. pediatric and uncooperative patients). This study was performed to evaluate the diagnostic performance and image quality of a novel EPI-based multi-contrast sequence compared to conventional sequences for the diagnosis of acute intracranial pathologies in the Emergency Department.METHODS:
190 consecutive brain MRI studies were obtained using a 1.5T GE SIGNA Artist MR scanner (GE Healthcare, Chicago, Illinois) including conventional brain MRI sequences and a recently developed multi-contrast EPI sequence (Multi-EPIMix1). T2W, T2 FLAIR, T1 FLAIR, GRE, ISO DWI, and ADC images were generated from the multi-contrast EPI sequence. The conventional brain MRI protocol included axial DWI, axial GRE, axial FLAIR and axial T2W sequences. The average acquisition time of the multi-contrast EPI sequence was 89 seconds (compared to at least 8 minutes and 13 seconds for the conventional sequences). Data collection was approved by the institutional review board. From these 190 cases, a sample of 30 cases was analyzed for the detection of DWI hyperintense lesions, intra-parenchymal or extra-axial foci of susceptibility signal, white matter and extra-axial FLAIR hyperintensities and intracranial masses. Images were also evaluated for the presence of motion artifacts and for their value in achieving the final imaging-based diagnosis.RESULTS:
10 cases (33.3%) showed DWI hyperintense lesions that were equally identified on both the multi-contrast EPI and conventional DWI sequences. 7 of these cases represented acute to subacute infarcts, 1 with demyelinating lesions and 2 cases with intracranial metastases. 9 cases showed intraparenchymal foci of susceptibility signal likely representing microhemorrhages. 1 of them showed a microhemorrhage in the multi-contrast EPI that was not seen in the conventional GRE sequence. 5 cases showed a better visualization of these lesions on the multi-contrast EPI. The number of white matter FLAIR hyperintensities identifiable on both FLAIR sequences was the same. 2 cases had intracranial masses that were equally seen in both non-contrast sequences. Motion artifacts were equal in 96.7% of cases and slightly worse in the conventional sequence in 1 case. Imaging-based diagnosis could be equally achieved in all cases.DISCUSSION:
Based on our preliminary findings, the multi-contrast EPI sequence had a similar diagnostic yield compared to conventional MR sequences with longer acquisition times. Clinically relevant acute intracranial pathologies seen in the emergency department (e.g. infarcts, intracerebral hemorrhage, white matter lesions, intracranial masses) were identified on both sequences suggesting that the rapid multi-contrast EPI sequence could be a potential diagnostic alternative in patients that cannot tolerate long MRI studies.CONCLUSION:
A rapid multi-contrast EPI-based sequence could provide a reasonable alternative for the clinical diagnosis of large intracranial pathologies in the emergency department in patients that cannot tolerate long MRI scans.Acknowledgements
We thank Stefan Skare for sharing the EpiMIX acquisition and reconstruction module.References
1. Skare S, Sprenger T, Norbeck O, et al. 1-minute full brain MR exam using a multicontrast EPI sequence. Magn Reson Med. 2018 Jun;79(6):3045-3054.Figures

Example of the different contrasts generated from the FEPIMix sequence.
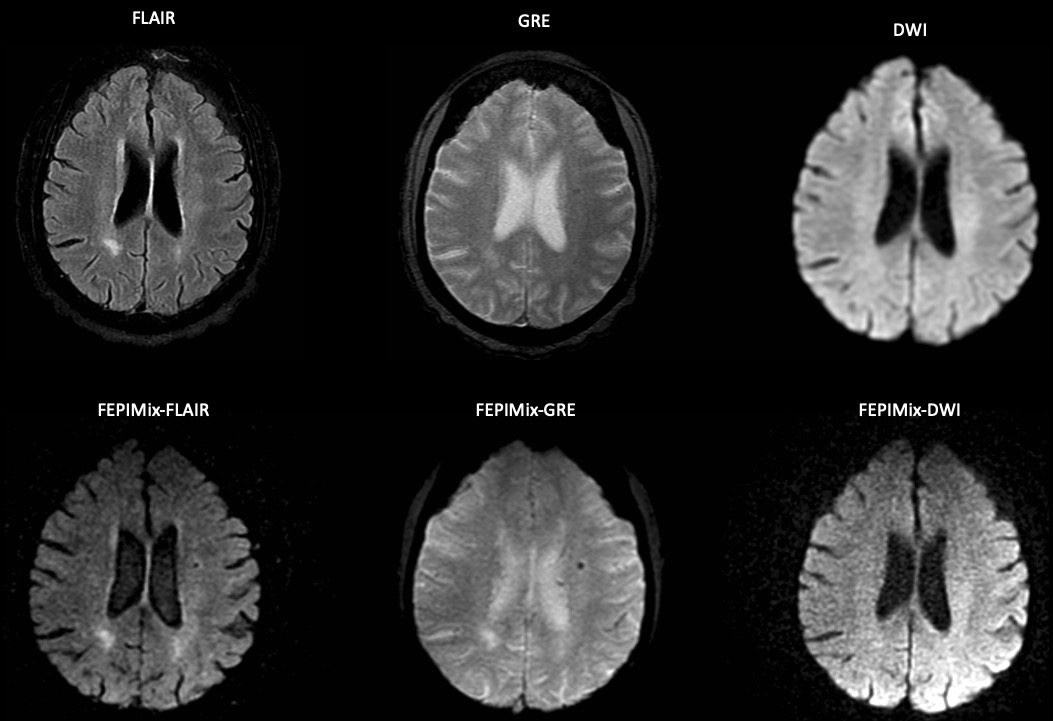
Comparison of conventional and FEPIMix sequences.