2983
Motion-Robust, Multi-Contrast Rapid Brain Screening Employing Single-Shot FSE with Variable Refocusing Flip Angle1Global MR Applications & Workflow, GE Healthcare, New York City, NY, United States, 2Global MR Applications & Workflow, GE Healthcare Canada, Vancouver, BC, Canada, 3Radiology, Columbia University, New York City, NY, United States
Synopsis
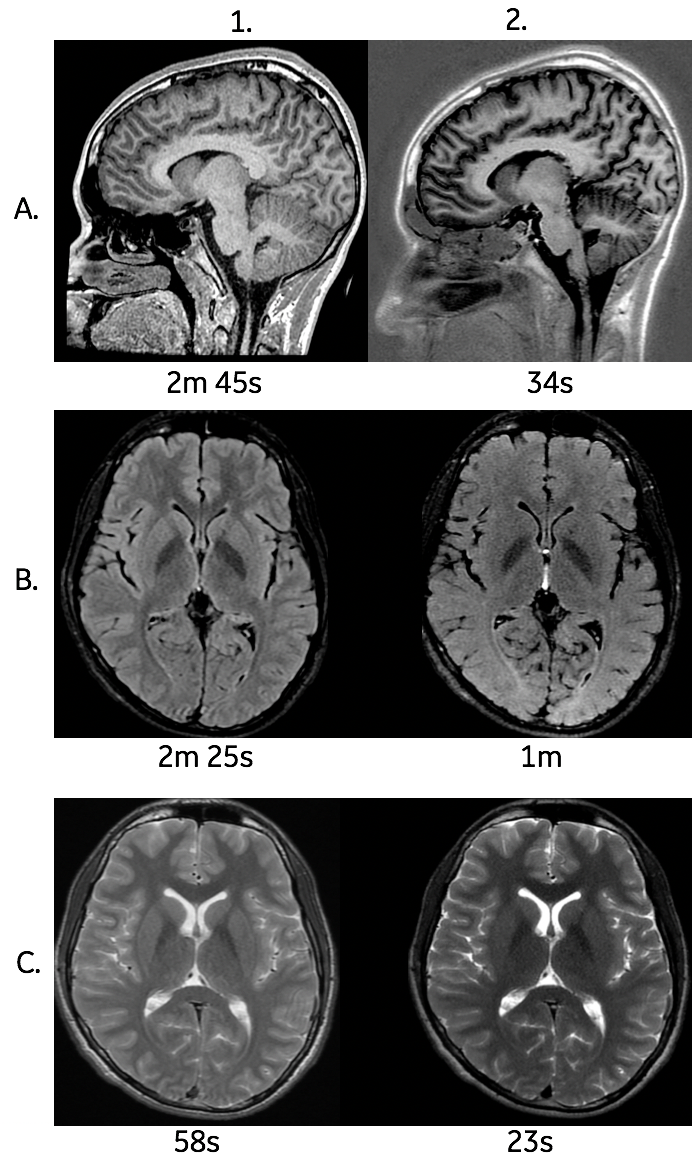
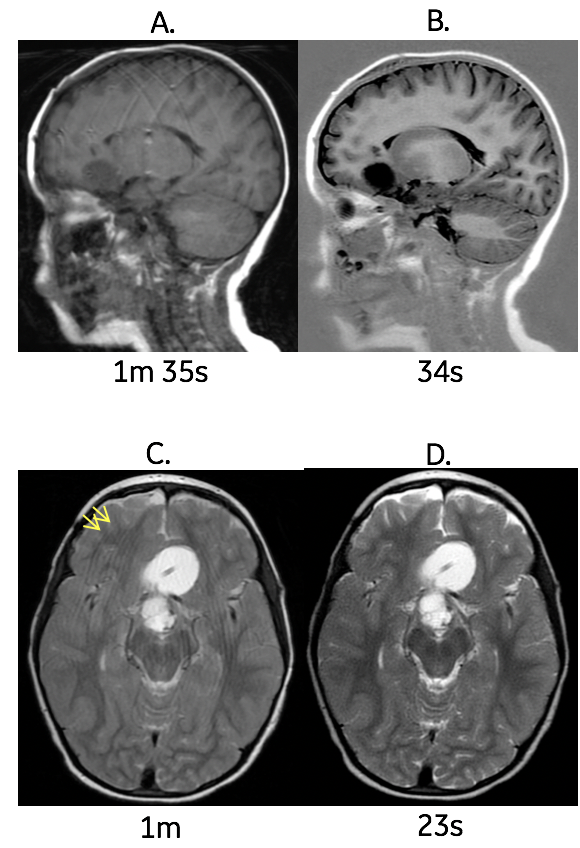
This study’s purpose was to compare single-shot with variable refocusing flip angle (vrfSSFSE) and standard multi-shot Fast Spin Echo (FSE) T1, FLAIR and T2w for pediatric brain evaluation. The resulting data shows in 5 subjects that vrfSSFSE provides clinically-acceptable diagnostic quality with a significant reduction in overall examination scan times and reduced motion/ghosting related artifacts typically observed with standard FSE imaging sequences.
Purpose:
Multi-contrast screening brain imaging is a commonly performed exam at most MRI pediatric facilities. Many of these exams require anesthesia to ensure the patient remains motionless during the collection of the data. However, the use of anesthesia comes at a significant cost to the patient along with other potential risk when sedating these patients for an exam that only take 30 minutes or less to complete. Often, due to many reasons, patients can’t receive anesthesia which means the patient is rescheduled for a different day/time or the exam is performed at that time without anesthesia. Performing these non-sedated exams with standard FSE sequences can lead to a suboptimal examination due to motion/ghosting. Other techniques, such as steady state imaging techniques, are used with good success for motion reduction, but have limitations reducing the overall confidence with this data1. As a result, the aim of this study is the assess the benefit vrfSSFSE to determine the effect of this technique on diagnostic capability, scan time impact and reduction of motion.Method:
In this IRB-approved study, we acquired T1, FLAIR and T2w images in 4 healthy volunteers and 1 patient, using standard FSE and an investigational vrfSSFSE pulse sequence. The study was performed on a 3T 70-cm bore MR scanner (Discovery MR750w, GE Healthcare, USA) using a GE Signa MRI Brain Array Coil (8 channel, High Resolution). The previously-described vrfSSFSE technique achieves improved T1 contrast via IR-preparation, centric view-ordering, refocusing flip angle optimization, and phase-sensitive inversion recovery image reconstruction2. T2w vrfSSFSE image quality is improved variable flip angle refocusing and full-Fourier acquisition3. Imaging parameters are described in Figure 1.
To evaluate diagnostic capability, two experienced radiologists performed blinded rating using the following 5-point scoring scale based off diagnostic quality, artifacts, uniformity, noise level and soft tissue contrast: 5 = Excellent (image quality excellent, suitable for diagnostic use), 4 = Good (image quality good, suitable for diagnostic use), 3 = Acceptable (image quality suitable for diagnostic use but with minor issues), 2 = Poor (image quality not completely suitable for diagnostic use) and 1 = Unacceptable (image quality not suitable for diagnostic use). Cohen’s kappa (k) statistic was used for the inter-rater reliability between the two readers.
Results & Discussion:
In total, the 5 subjects acquired for this review, both radiologist scored this data independetly with a inter-rater k score of 0.88. The vrfSSFSE images received an average score of 3.5 (Good) overall diagnostic quality to include reduction of motion artifacts for each contrast-weighted image. The vrfSSFSE FLAIR sequence scored the lowest due to limited suppression of CSF at the base of the skull and reduced contrast, making it a challenge to determine gray/white matter borders compared to the standard FLAIR images.
A few challenges remain, including increasing gray/white matter contrast and CSF suppression artifacts on the vrfSSFSE T2 FLAIR, and mitigating the effects of patient motion for T1 vrfSSFSE that may occur during the inversion time (TI). Scan times may be further reduced for T1 vrfSSFSE by interleaving the inversion recovery (IR) preparation and readout for multiple slice locations, as in standard multi-shot FSE.
Conclusion:
In this work, we have demonstrated the benefits of rapid, single-shot imaging for screening non-sedated pediatric patients to reduce motion artifacts and the need for sedation. The vrfSSFSE sequence appears to be a very promising technique when added in the right clinical situation to great reduction exam time and patient motion while maintaining acceptable image quality. Future work will include the collection of more clinical data of non-sedated children to fully understand the clinical diagnostic capabilities over a wide range of patients and pathologies.Acknowledgements
No acknowledgement found.References
1: Rozovsky, Katya et al. Fast-brain MRI in children is quick, without sedation, and radiation-free, but beware of limitations. Journal of Clinical Neuroscience 12/2012; 20(3). · DOI:10.1016/j.jocn.2012.02.048
2: Litwiller, D et al. Fast, Motion-Robust, T1-Weighted Neuro Imaging with Single-Shot Fast Spin Echo. Proceedings of the American Society of Neuroradiology (ASNR), 2018, Vancouver, BC, Canada.
3: Vigen, K et al. Fast Neuro MRI with Variable Refocusing Flip-Angle 2D SSFSE. International Society for Magnetic Resonance in Medicine (ISMRM) 2017:
4: Ma J. Multislice and multicoil phase-sensitive inversion-recovery imaging. Magn. Reson. Med. 2005;53:904–910.
5: Hou P, et al. Phase-sensitive T1 inversion recovery imaging: a time-efficient interleaved technique for improved tissue contrast in neuroimaging. AJNR Am J Neuroradiol 2005;26:1432–1438.
Figures