2982
Development of an Express MRI Protocol for Pediatric Brain Imaging in a Clinical Setting1GE Healthcare, Brooklyn, NY, United States, 2Radiology, New York Presbyterian Hospital, New York City, NY, United States, 3Radiology, Columbia University, New York City, NY, United States
Synopsis
The purpose of this study was to develop a routine express MRI protocol for pediatric brain imaging that would provide consistent and robust image quality in one-fourth the scan time of current industry standard protocols, utilizing Fast Spin Echo (FSE) T1, FLAIR, T2w, Gradient Echo (GRE) T2*, and Diffusion Weighted Echo Plane Imaging (DW-EPI) sequences. Evaluation was performed on a group of 20 patients and results indicated that imaging using the express brain protocol was of clinically sufficient diagnostic quality and allowed for a significant reduction in overall scan times compared to industry standard routine brain imaging protocols.
Purpose:
MRI has been proven extremely valuable when imaging the brain to assist in visualizing and diagnosing many abnormalities in children around the world. When performing this type of exam, like any other MR scan, it’s essential that data is free of motion/ghosting artifacts to make an accurate clinical diagnosis which means most exams for children are performed with sedation. However, the use of anesthesia comes at a significant cost along with other potential risk when sedating these patients. This also produces extremely long (> 45 minutes) exam times which ties up the MR resource reducing the number of patients that can be examined in a given day and reducing overall utilization and operational efficiency in the department. Many facilities have made attempts to improve on system utilization while trying to reduce amount of time a patient is under sedation with adjustments to standard protocol or newer sequences to replicated a particular contrast, but this comes at cost to quality, consistency and overall diagnostic capabilities due to limitations with those changes1. As a result, the aim of this study is the assess the benefit non-research clinical sequences to develop a reduced scan-time express protocol with no significant compromise of diagnostic capability and quality.Methods:
In this study, we acquired standard routine brain and the newly develop express brain protocol for FSE sagittal T1, axial FLAIR, axial T2w, axial GRE T2* and axial DW-EPI sequences in 20 patients. The study was performed on, 3T 70cm bore MR scanners (Discovery MR750w, GE Healthcare, USA) using GE Signa MRI Brain Array Coil (8 channel, High Resolution). All data was collected without gadolinium contrast focusing on the core imaging sequences prior to the administration of contrast. Imaging parameters are described in Figure 1.
To evaluate diagnostic capability, two experienced radiologists performed blinded rating using the following 5-point scoring scale based off diagnostic quality, artifacts, uniformity, noise level and soft tissue contrast: 5 = Excellent (image quality excellent, suitable for diagnostic use), 4 = Good (image quality good, suitable for diagnostic use), 3 = Acceptable (image quality suitable for diagnostic use but with minor issues), 2 = Poor (image quality not completely suitable for diagnostic use) and 1 = Unacceptable (image quality not suitable for diagnostic use). Cohen’s kappa (k) statistic was used for the inter-rater reliability between the two readers.
Results & Discussion:
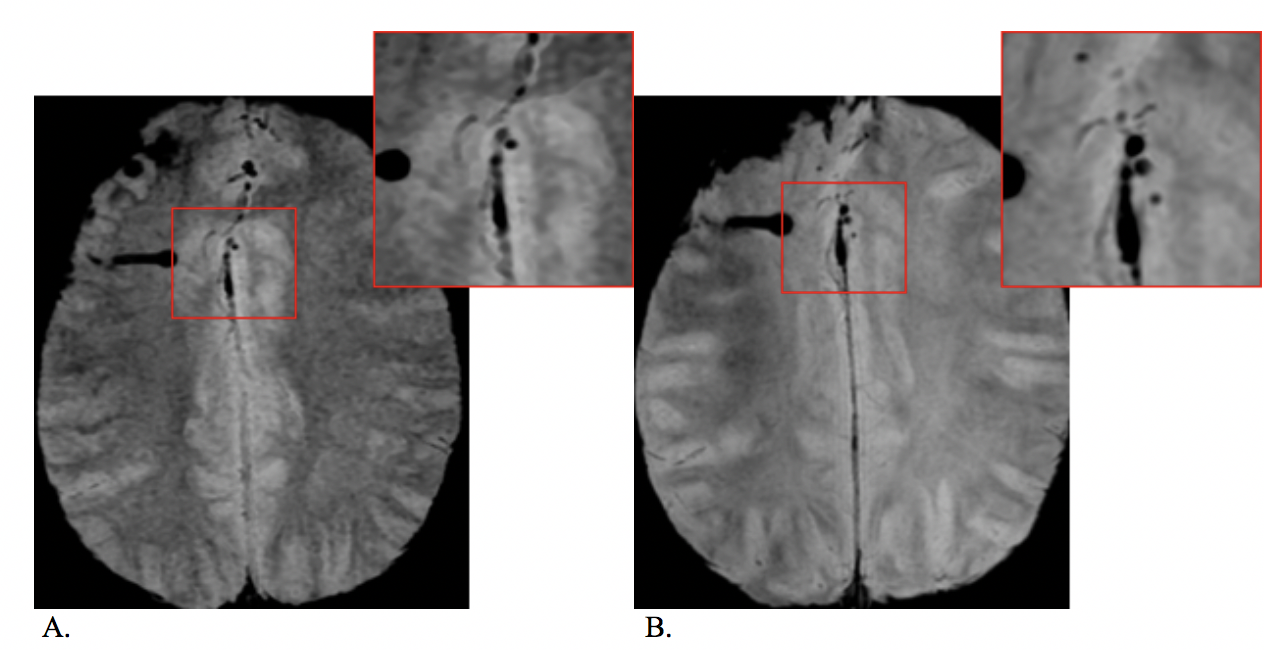
In the total of the 20 subjects acquired for this review, both radiologist scored this data independently with a inter-rater k score of 0.81. The express brain protocol received an average score of 3.8 (Good) or better for overall diagnostic quality compared to that of the standard protocol which received an average of 4.8 (Good to Excellent) for overall quality. Figure 2 shows a direct image quality sample comparison between the two protocols. This scoring added with radiologist feedback shows that the images acquired with the express brain protocol can provide the needed diagnostic capabilities for most brain studies at a fraction of the time of standard imaging sequences. Overall, the express protocol scored lower in resolution especially on the T2* GRE and T1 contrast sequence which are both 2D compared to that of 3D data for the standard protocol. Figure 3 depicts that the 3D T2* susceptibility weighted images shows more smaller blood products compared to the 2D version of this sequence. Each radiologist also commented on slightly lower SNR on the express protocol which factored into the lower average score compared to the standard protocol. This shows there is a correlation between scan time reduction and image score. The average scan time decrease from average of 15m 40s (standard) to 4m 25s (express) shows close to a 73% decrease in overall scanning time.
There are still a few remaining challenges: If higher resolution is desired, the impact to scan time is a significant increase especially on FLAIR and GRE T2* sequences. Patient motion will still be a factor with this express protocol even with the significant scan time reduction. Defining a similar protocol for 1.5T systems that will deliver the same impact to scan time with little to know reduction to diagnostic quality.
Conclusion:
In this work, we demonstrated that express brain protocols can provide similar diagnostic capabilities compared to routine standard protocols with one-fourth of the scan time. This reduction allows for significant increase in scanner utilization, operational efficiency and overall time the patient may need to be sedated. This protocol can also be adopted to many other brain related protocols/exams to reduce scan time allowing more focus to other sequences for a specific exam such as imaging the Internal Auditory Canal, Cranial Nerves, Optic Nerve and Hippocampus.Acknowledgements
No acknowledgement found.References
1: Rozovsky K, Ventureyra EC, Miller E. Fast-brain MRI in children is quick, without sedation, and radiation-free, but beware of limitations. J Clin Neurosci. 2013 Mar;20(3):400-5. doi: 10.1016/j.jocn.2012.02.048. Epub 2012 Dec 21. PubMed PMID: 23266077.Figures