2975
Simultaneous Multi-Slice Spin and Gradient Echo Dynamic Susceptibility-Contrast Perfusion Imaging of Gliomas1Radiology and Biomedical Imaging, University of California, San Francisco, San Francisco, CA, United States, 2Applications and Workflow, GE Healthcare, Waukesha, WI, United States, 3Applications and Workflow, GE Healthcare, Orsay, France, 4Applications and Workflow, GE Healthcare, Menlo Park, CA, United States
Synopsis
DSC MRI allows for the characterization of first-pass hemodynamics by measuring signal intensity variation resulting from susceptibility changes during the injection of a paramagnetic contrast agent. Simultaneous spin and gradient-echo (SAGE) DSC MRI sequences can provide perfusion parameters that are sensitive to both microvasculature and larger vessels facilitating the measurement of vessel size and correcting for T1 leakage effects. This work evaluates the integration of SAGE EPI with a simultaneous multi-slice excitation to attain high temporal resolution DSC perfusion with full brain coverage. Two protocols with different multi-band acceleration factors were compared in patients with glioma.
Introduction
Dynamic susceptibility contrast (DSC) MRI allows for the characterization of first-pass hemodynamics such as relative cerebral blood volume (CBV) by measuring signal intensity variation due to susceptibility variations during the injection of a paramagnetic contrast agent. Simultaneous spin and gradient-echo (SAGE) DSC MRI sequences1-3 have been introduced to improve clinical utility by providing quantitative metrics thatreflect vessel size4-5 and allow for the correction of T1 leakage effects.6-7 However, the extra time required for the spin echoe results in either decreased temporal resolution or reduced brain coverage. This work evaluates the integration of SAGE echo-planner imaging (EPI) with a simultaneous multi-slice (SMS) excitation including blipped-controlled aliasing in parallel imaging (blipped-CAIPI)8 and ARC-based acceleration in-plane to attain high temporal resolution with full brain coverage. Whereas prior studies have used SMS approaches to increase the temporal resolution resulting in elevated noise in the ΔR2* curves, our protocol was designed to maintain accurate quantification and integrate with online scanner reconstruction. Dynamic signal-to-noise ratio (dSNR) of the ΔR2* and ΔR2 time curves and rCBV maps were compared between two protocols with different multi-band acceleration (MUX) factors in patients with glioma.Methods
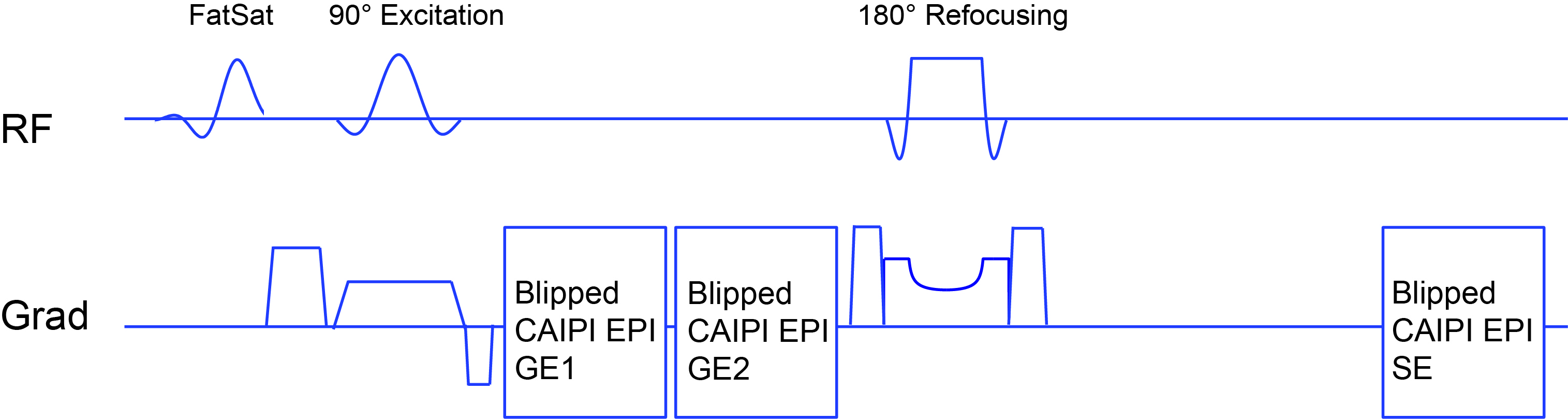
A commercial version of a 2D blipped-CAIPI gradient-echo (GE) EPI sequence with interleaved multi-slices acquisition (Hyperband EPI) was extended to allow for the simultaneous acquisition of two GEs before the 180° refocusing pulse and one spin-echo (SE) after the refocusing pulse (Figure 1). MB-SAGE-DSC perfusion imaging was performed using a GE 3T MR 750 scanner (GE Healthcare, Waukesha, WI) and 32 channel receive-only head coil (NovaMedical) with either a MUX factor of two or three (13 patients each) during the injection of Gd-DTPA contrast agent with 15s delay. The imaging parameters common to both protocols included a 24x24cm2 FOV, 100x100 matrix size, 3mm slice thickness, in-plane acceleration factor of two, and TE1/TE2/TE3=8.6/30/100ms. For a MUX factor of 2, 24 slices, 1.72s TR, and 70 temporal points were prescribed while the protocol with a MUX factor of 3 acquired 33 slices with a 1.5s TR, and 80 time points. A separate reference scan was collected prior to the DSC scan to apply to the SE echoes during the reconstruction. In-plane ARC-based9 and slice-GRAPPA10 reconstruction were performed using external coil calibration data.
From the signal intensity values at three TEs, ΔR2* and ΔR2 curves were derived while removing T1 leakage effects as in Stokes et al.7 R2* and R2 baseline value were estimated from six time points acquired prior to contrast injection after steady-state was reached. dSNR was defined as the peak height of ΔR2*/ΔR2 curves divided by the standard deviation measured before the arrival of contrast agent.11 Mean dSNR within segmented normal-appearing white matter (NAWM) regionswas calculated. rCBV was determined separately using ΔR2* or ΔR2 curves and normalized for each patient. Maps of mean vessel diameter (MVD) were generated as the ratio of the integrals of ΔR2*(t) and ΔR2(t) over the first-pass bolus.2,7
Results
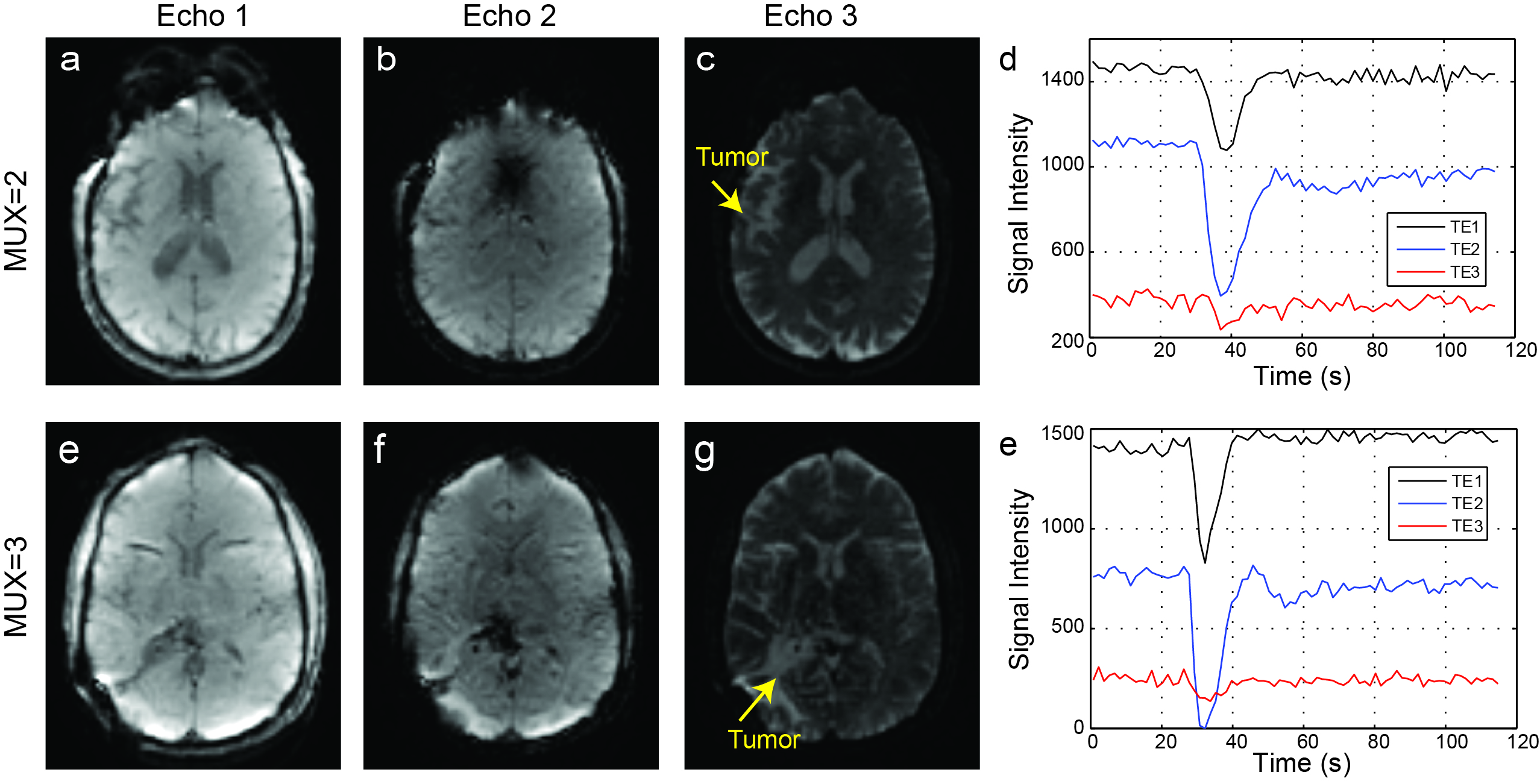
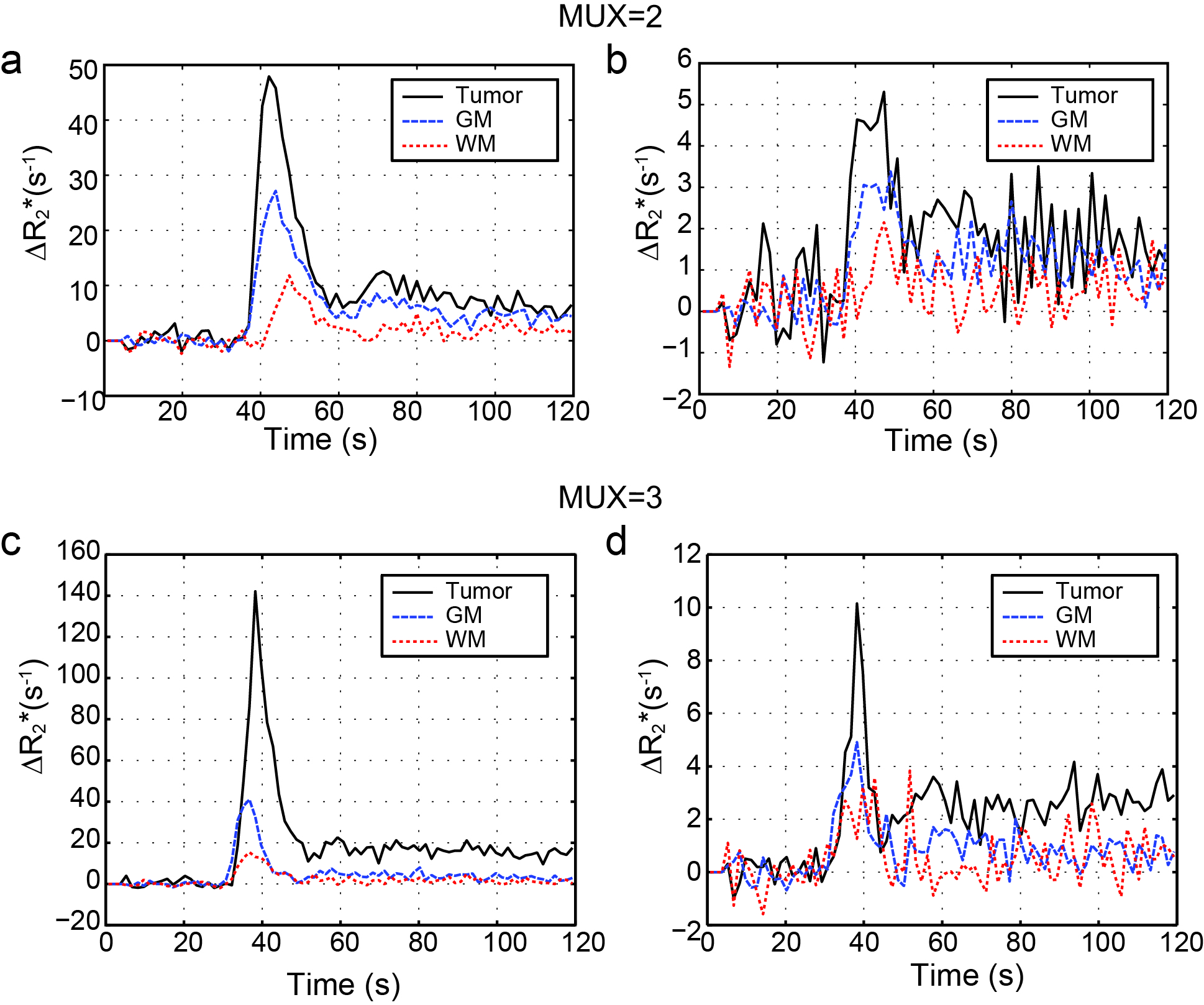
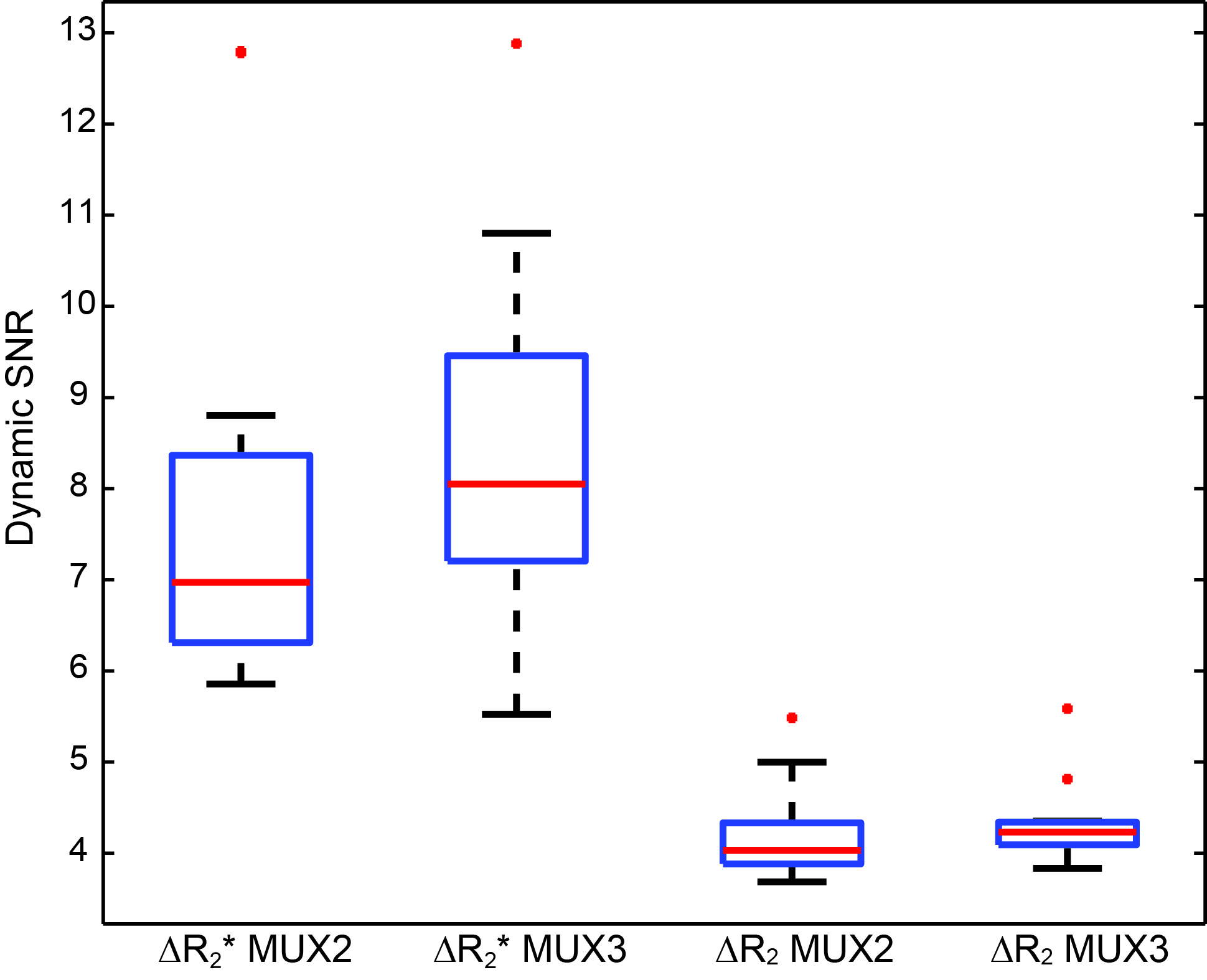
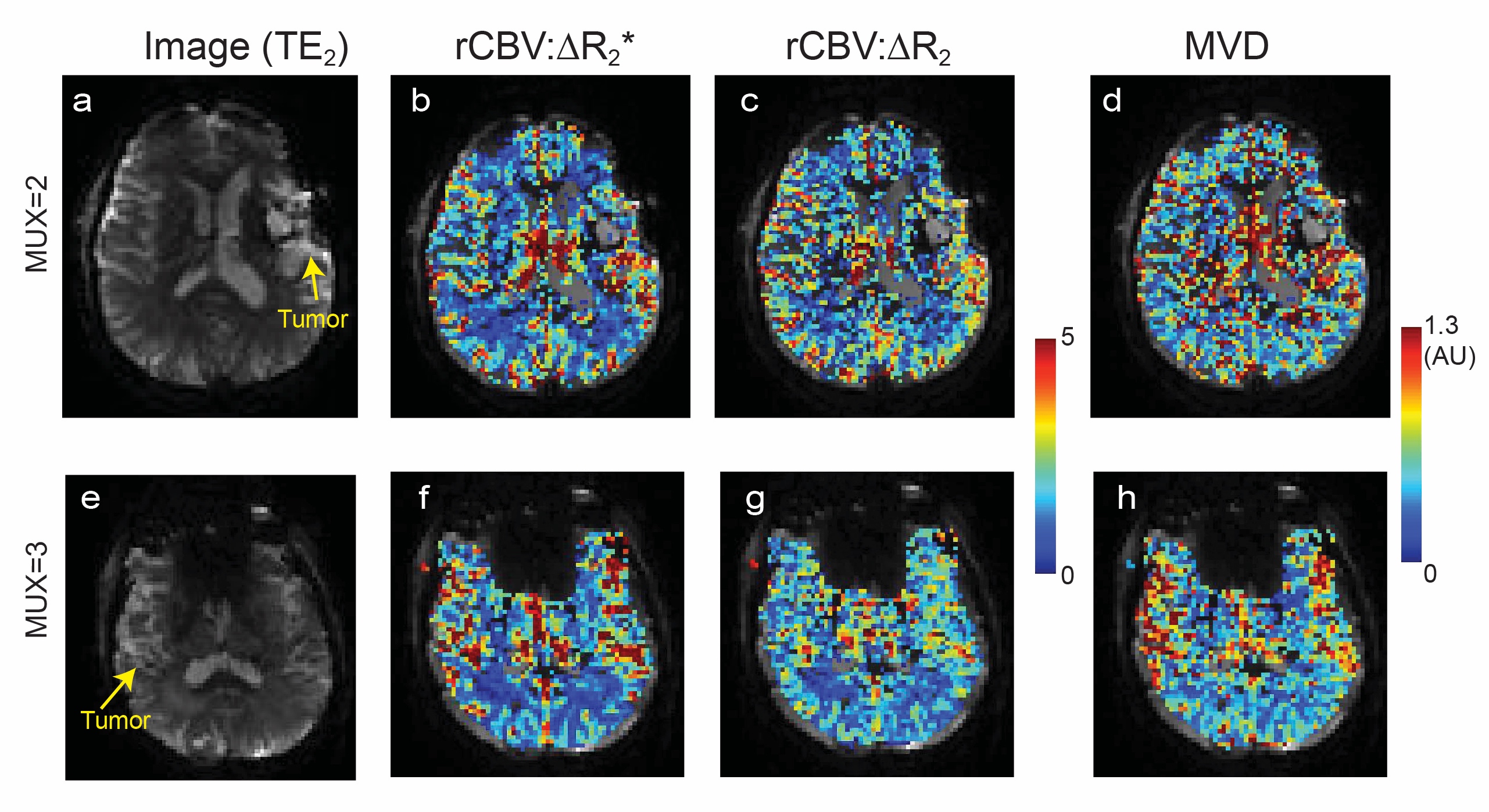
Figure 2 shows pre-bolus images for each echo from two patients, and corresponding time curves from a voxel within residual tumor. With both MUX factors, no visible aliasing artifacts were observed. Figure 3 shows ΔR2*(t) and ΔR2*(t) time curvesfrom pixels in tumors, normal gray matter, and NAWM, from the same patient displayed in Figure 2. ΔR2 and ΔR2* curves return to baseline, indicating that T1 leakage effects are properly corrected. A comparison of dSNR in ΔR2*(t) and ΔR2(t) curves in white matter over 13 patients for each protocol is presented in Figure 4. dSNRs between the two protocols are not significantly different. Figure 5 demonstrates the rCBV maps calculated from ΔR2*(t) and ΔR2(t) and MVD from two patients post-surgical resection scanned with the different protocols. Overall depiction of the NAWM and gray matter are visually similar between protocols. Differences between ΔR2*-based and ΔR2-based rCBV can be observed within the lesion; the MVD is elevated in residual tumor.Conclusion
Combining SAGE and blipped-CAIPI multi-slice acquisition allows for a 1.5-1.7 s temporal resolution with 2.4 mm in-plane resolution and full brain coverage for DSC perfusion imaging. No significant aliasing artifacts were present despite the use of external calibration data during reconstruction. Our mean dSNRs in NAWM with the two different protocols having different MUX factors were similar, indicating a MUX factor of three can be reliability used for brain DSC MRI, allowing full brain coverage at a 3 mm slice resolution. Acquiring two GEs and a SE, allows for quantification of additional metrics that may be more sensitive to subtle changes in microvasculature structure due to treatment while simultaneously correcting T1 leakage effects.Acknowledgements
This work was supported by GE Healthcare.References
[1] Schmiedeskamp H, Straka M, Newbould RD, Zaharchuk G, Andre JB, Olivot JM, Moseley ME, Albers GW, Bammer R. Combined spin‐and gradient‐echo perfusion‐weighted imaging. Magn Reson Med 2012;68(1):30-40.
[2] Donahue KM, Krouwer HG, Rand SD, Pathak AP, Marszalkowski CS, Censky SC, Prost RW. Utility of simultaneously acquired gradient‐echo and spin‐echo cerebral blood volume and morphology maps in brain tumor patients. Magnetic Magn Reson Med 2000;43(6):845-853.
[3] Skinner JT, Robison RK, Elder CP, Newton AT, Damon BM, Quarles CC. Evaluation of a multiple spin- and gradient-echo (SAGE) EPI acquisition with SENSE acceleration: applications for perfusion imaging in and outside the brain. Magn Reson Imaging 2014;32(10):1171–80.
[4] Kiselev VG, Strecker R, Ziyeh S, Speck O, Hennig J. Vessel size imaging in humans. Magn Reson Med 2005;53(3): 553–563.
[5] Lemasson B, Valable S, Farion R, Krainik A, Remy C, Barbier EL. In vivo imaging of vessel diameter, size, and density: a comparative study between MRI and histology. Magn Reson Med 2013;69(1):18–26.
[6] Paulson ES, Schmainda KM. Comparison of dynamic susceptibility-weighted contrast-enhanced MR methods: recommendations for measuring relative cerebral blood volume in brain tumors. Radiology 2008; 249(2):601-13.
[7] Stokes AM, Quarles CC. A simplified spin and gradient echo approach for brain tumor perfusion imaging. Magn Reson Med 2016;75(1):356-362.
[8] Setsompop K, Gagoski BA, Polimeni JR, Witzel T, Wedeen VJ, Wald LL. Blipped‐controlled aliasing in parallel imaging for simultaneous multislice echo planar imaging with reduced g‐factor penalty. Magn Reson Med 2012; 67(5):1210-1224.
[9] Beatty PJ, Brau AC, Chang S, Joshi SM, Michelich CR, Bayram E, Nelson TE, Herfkens RJ, Brittain JH. A method for autocalibrating 2-D accelerated volumetric parallel imaging with clinically practical reconstruction times. In: Proceedings of the 15th Annual Meeting of ISMRM, Berlin, Germany, 2007. p. 1749.
[10] Cauley SF, Polimeni JR, Bhat H, Wald LL, Setsompop K. Interslice leakage artifact reduction technique for simultaneous multislice acquisitions. Magn Reson Med 2014;72(1):93-102.
[11] Lupo JM, Lee MC, Han ET, Cha S, Chang SM, Berger MS, Nelson SJ. Feasibility of dynamic susceptibility contrast perfusion MR imaging at 3T using a standard quadrature head coil and eight‐channel phased‐array coil with and without SENSE reconstruction. J Magn Reson Imaging 2006. 24(3):520-529
Figures