2972
Rapid Volumetric Imaging of the Spinal Cord using AMIRA-3D1Dept. of Biomedical Engineering, University of Basel, Allschwil, Switzerland, 2Dept. of Radiology, Radiological Physics, University of Basel Hospital, Basel, Switzerland
Synopsis
For fast volumetric spinal cord imaging, a 3D acquisition strategy for the recently published Averaged Magnetization Inversion Recovery Acquisitions (AMIRA) approach was developed: AMIRA-3D. It typically acquires 12 slices with a resolution of 0.67 x 0.67 x 3.0 mm3 in 5:27 min, which represents an acquisition time of just 27 secs per slice. As common to all AMIRA approaches, images with remarkable different tissue contrast are acquired for each slice (or partition) simultaneously. Some of these images can be combined to both enhance and fine-tune the desired tissue contrast.
Introduction
In the past years, several MRI approaches have been developed and investigated that tried to improve spinal cord (SC) imaging 1. Particularly, sequences dedicated to SC morphometry struggle with challenges like motion, fine structures and the typically low contrast between gray matter (GM) and white matter (WM) in the spinal cord 1. The favorite phase-sensitive inversion recovery (PSIR) approach has facilitated important results 2-3, but as a 2D sequence its efficiency is limited 2-3, and the corresponding 3D variant needs long acquisition times 4.
Recently, the Averaged Magnetization Inversion Recovery Acquisitions (AMIRA) approach was presented 5, which simultaneously acquires images of different contrast for each slice. Furthermore, these images can be combined to enhance signal and contrast to noise ratio 5. Despite the benefits, the original AMIRA approach – as a 2D acquisition strategy – lacks the advantages of a 3D sequence such as a closed acquisition volume and a usually higher acquisition efficiency per unit time. In the following, the development of a complete three-dimensional AMIRA acquisition technique is presented (AMIRA-3D). AMIRA-3D achieves typical resolutions of 0.67 x 0.67 x 3.0 mm3 in 27 secs per slice, while preserving the common AMIRA benefits such as contrast fine-tuning by image combination.
Methods
AMIRA-3D sequence
The basic idea of the AMIRA approach is to sample the transient response function towards the steady state of a balanced steady state free precession (bSSFP) sequence after an initial inversion recovery (IR) preparation 5. Several images with different effective inversion times TI are acquired in segments in a time-limited cine approach along the recovery curve 5. For the present 3D variant (c.f. Figure 1), the cine-like sampling of multiple, segmented images after an IR preparation was realized within a manufacturer supplied bSSFP sequence with linear view orderings in a 3D acquisition mode. Four saturation slices were also added (details below).
General parameters
FOV = 128 x 128 mm2, resolution = 0.67 x 0.67 x 3.0 mm3, matrix = 192 x 192 x 12, 33% slice oversampling, 12 k-space lines per segment, phase partial Fourier = 4/8, slice partial Fourier = 6/8, TRbSSFP = 6.55 ms, TEbSSFP = 3.12 ms, bandwidth = 310 Hz/Px, flip angle = 40 deg. A global, adiabatic inversion pulse was used. Seven images with the effective TI = [170.0, 248.6, 327.2, 405.8, 484.4, 563.0] ms were acquired. Two saturation slices were defined adjacent and parallel to the acquisition volume, one in head and one in feet direction each. Two further saturation slices resided left and right, parallel to the course of the SC. They were also orthogonal to the first two saturation slices described before.
Measurements
Proof of concept acquisitions were performed at the cervical SC of volunteers (c.f. Results section). All experiments were performed on a 3T whole-body MR system (Siemens Magnetom Prisma) using a 64-channel phased array head and neck coil.
Results
Figure 2 depicts an example for the seven images acquired simultaneously in each slice / partition with the suggested AMIRA-3D technique from Figure 1. The sample images demonstrate the typical contrast variation known from common 2D AMIRA acquisitions 5. Based on previous AMIRA developments and quantitative investigations, Figure 3 illustrates that another main characteristic of the AMIRA approach is unchanged: image combinations allow the adaptation and possible enhancement of tissue contrast. These prospects 'come for free', i.e., no additional measurements or changes thereof are required.
Figure 4 shows the full image set of an AMIRA-3D acquisition, the image combinations optimized for GM-WM contrast. Using the peripheral saturation slices, AMIRA-3D provides very similar signal stability and the same basic resolving capability as the original AMIRA-2D, yet, with a considerably increased slice resolution by almost 3x in merely half the acquisition time per slice.
Figure 5 depicts the same AMIRA-3D acquisition; however, the image combinations are tuned to a strong cerebrospinal fluid (CSF) to soft tissue contrast now.
Discussion and Conclusion
The successful realization of a 3D AMIRA technique for high SC imaging
quality could be demonstrated. Compared to the original 2D approach, AMIRA-3D still
achieves a considerable gain in acquisition efficiency: Typically, 12 slices
with an in-plane resolution of 0.67 x 0.67 mm2 and merely 3.0 mm
slice thickness are acquired in 27 secs per slice only. The multiple
tissue contrasts at hand are of particular value for further image
postprocessing like tissue segmentation and allow dedicated contrast
adaptations that were also eponymous for the whole AMIRA approach.Acknowledgements
No acknowledgement found.References
1. Stroman PW, Wheeler-Kingshott C, Bacon M et al. The current state-of-the-art of spinal cord imaging: Methods. Neuroimage 2014; 84:1070-1081.
2. Papinutto N, Schlaeger R, Panara V et al. 2D phase-sensitive inversion recovery imaging to measure in vivo spinal cord gray and white matter areas in clinically feasible acquisition times. J Magn Reson Imaging 2015; 42:698-708.
3. Schlaeger R, Papinutto N, Panara V, et al. Spinal Cord Gray Matter Atrophy Correlates with Multiple Sclerosis Disability. Annals of Neurology 2014; 76:568–80.
4. Kearney H, Mieszkiel KA, Yiannakas MC et al. A pilot MRI study of white and grey matter involvement by multiple sclerosis spinal cord lesions. Multiple Sclerosis 2013; 2:103-108.
5. Weigel M, Bieri O. Spinal cord imaging using averaged magnetization inversion recovery acquisitions. Magn Reson Med 2018; 79:1870-1881
Figures

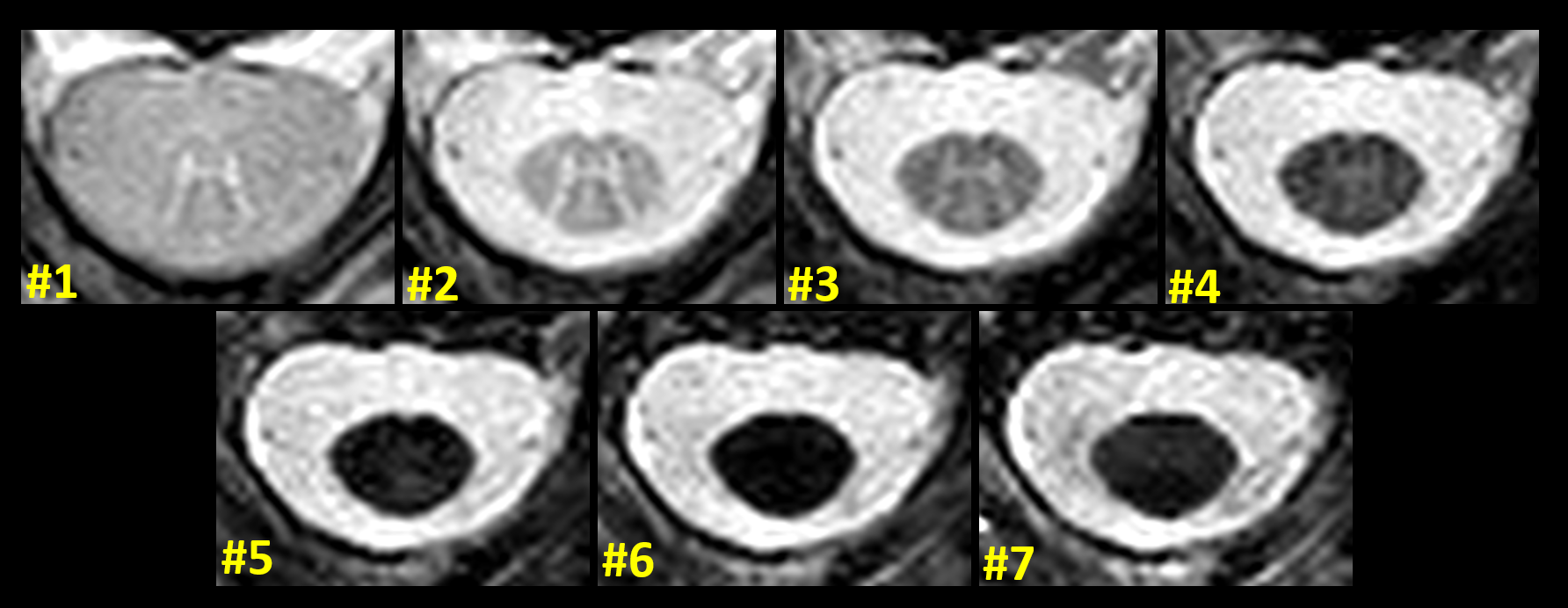
Figure 2: Representative example for the seven images simultaneously acquired for each slice in the 3D slab volume, shown in chronological order from lowest to highest TI. Image #1 displays the highest GM-WM contrast, whereas image #7 displays the highest WM to cerebrospinal fluid (CSF) contrast. As has been shown for the original AMIRA-2D approach, this interesting effect is based on the different transient signal responses of the three tissues during a bSSFP readout (after IR preparation).
The slice was located at the spinal disc C2-3.
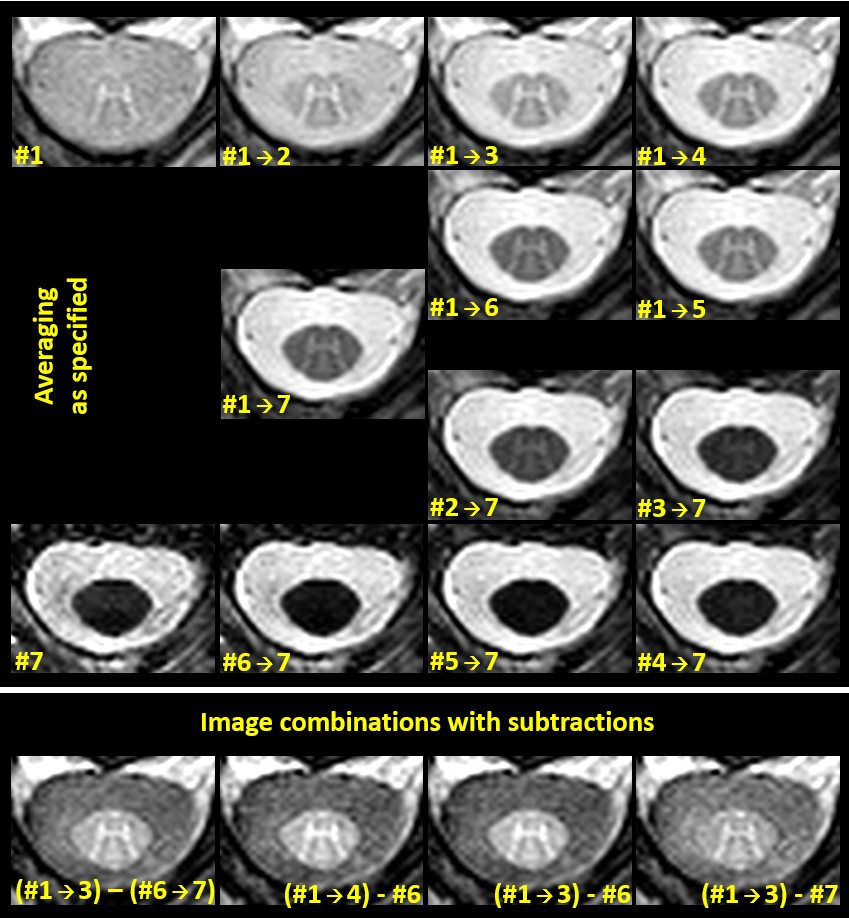
Figure 3: One of the main characteristics of the generic AMIRA approach is the potential of image combination 5. The upper panel demonstrates that this interesting property is preserved for the new 3D approach: Starting with image #1 with the highest GM-WM contrast (top-left), the images #2 to #7 are successively averaged up in ascending order to analyze the contrast changes, as labeled.
Upper panel, bottom left: Starting with image #7 with the highest WM-CSF contrast, the images #6 to #1 are successively averaged up in descending order.
Lower panel: Examples for further image combinations with reduced CSF signal intensity. Combinations as specified.
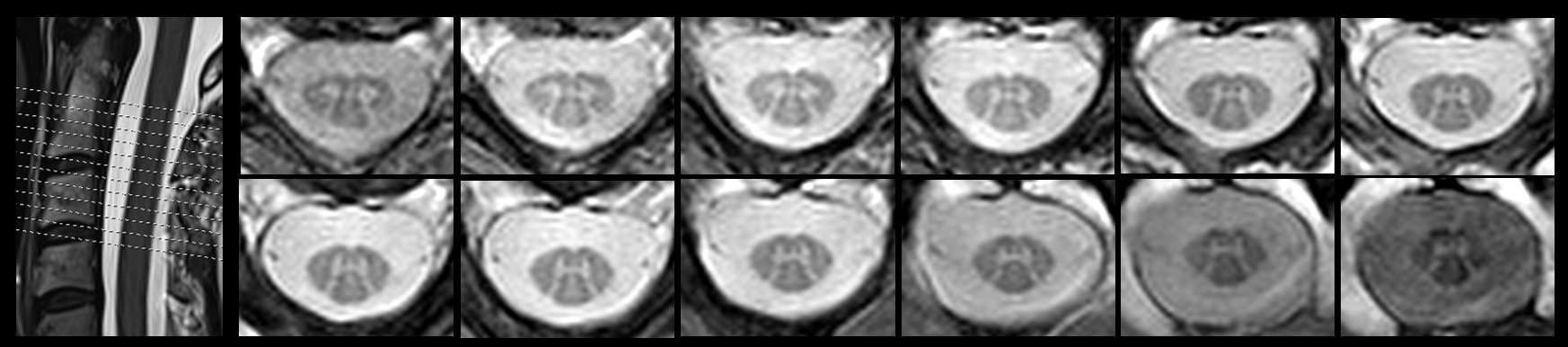
Figure 4: The suggested AMIRA-3D approach acquires 12 slices of 0.67x0.67mm2 with 3.0mm slice thickness in 5:27min. Here, an acquisition along the cervical spine approximately between discs C1-2 and C3-4 is depicted. The acquisitions demonstrate a good image quality over the whole slab. For improved signal and GM-WM structure enhancement, always the first four images (#1 to #4) of the AMIRA acquisition were averaged for each slice.
It should be noted that all slices are displayed with identical conditions for the window-levelling. Changes in signal intensity for the peripheral slices are residual effects of the slab excitation profile; however, the tissue contrast remains good.
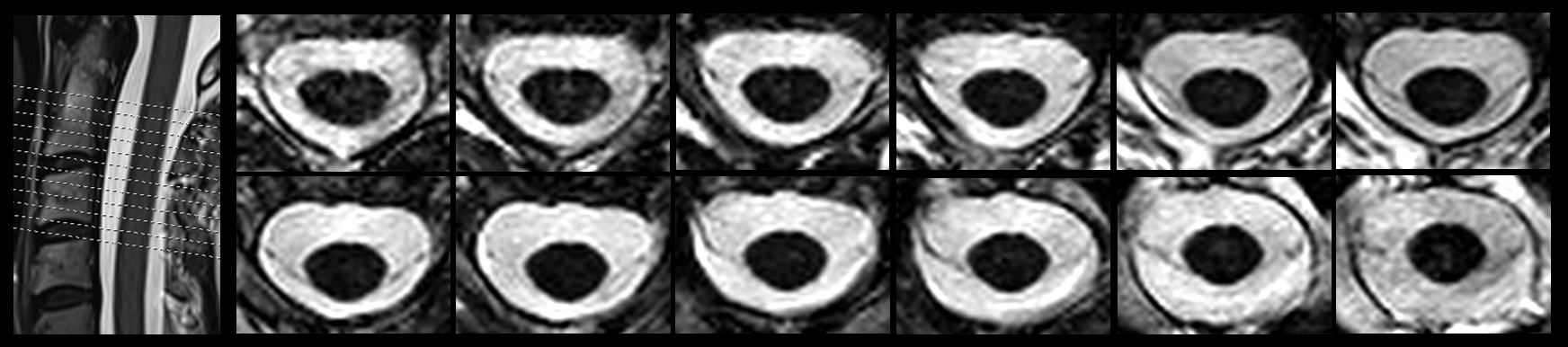
Figure 5: Display of the same cross-sectional slices as in Figure 4; however, always the last three images (#5 to #7) of the same AMIRA-3D acquisition were averaged to generate images with strong CSF to soft tissue contrast for each slice. The displayed images are well-suited for volumetric approaches.
Again, it should be noted that Figures 4 and 5 are based on the same acquisition and that no additional measurements are necessary.