2970
Comparison of AIR Coil Technology to Conventional Head Coils for Neuro Imaging1Radiology, Mayo Clinic, Rochester, MN, United States, 2GE Healthcare, Aurora, OH, United States, 3GE Healthcare, Waukesha, WI, United States
Synopsis
A 16-channel head coil using novel Adaptive Image Receive (AIR) technology was compared to 8-channel and 32-channel head coils on the Compact 3T system in nine healthy subjects using MPRAGE, FLAIR, GRE, and T2 FSE pulse sequences. Two neuroradiologists graded the AIR coil against the 8-channel and 32-channel coils on signal-to-noise ratio, gray-white matter contrast, lesion depiction, artifact, and overall image quality. On average the AIR coil performed similar to the 8-channel head coil, though not as well as the 32-channel coil. This study demonstrates feasibility of AIR coil technology for imaging of the brain and denotes areas on which future coil designs may improve.
Introduction
Multi-element receive-only coils continue to evolve providing improved signal-to-noise ratio (SNR) and performance for advanced imaging applications. Limitations of coil performance include patient ergonomic fit and requirements for fixed coil geometries. These limitations are being addressed with the development of Adaptive Image Receive (AIR) coils (GE Healthcare, Waukesha, WI, USA) (1,2) in which the effects of capacitive coupling and mutual inductance between coil elements are reduced, allowing for a higher coil density and flexible coil fit. At our institution this technology has been implemented for imaging the brain on the Compact 3T (C3T) system (3-5), which offers additional opportunities for sequence development owing to its high-performance gradients. The purpose of this work is to demonstrate feasibility of the AIR coil technology for brain imaging by comparing the performance of a 16-channel AIR coil based on an open, ski-mask design with conventional 8-channel and 32-channel head coils on the C3T system.Methods
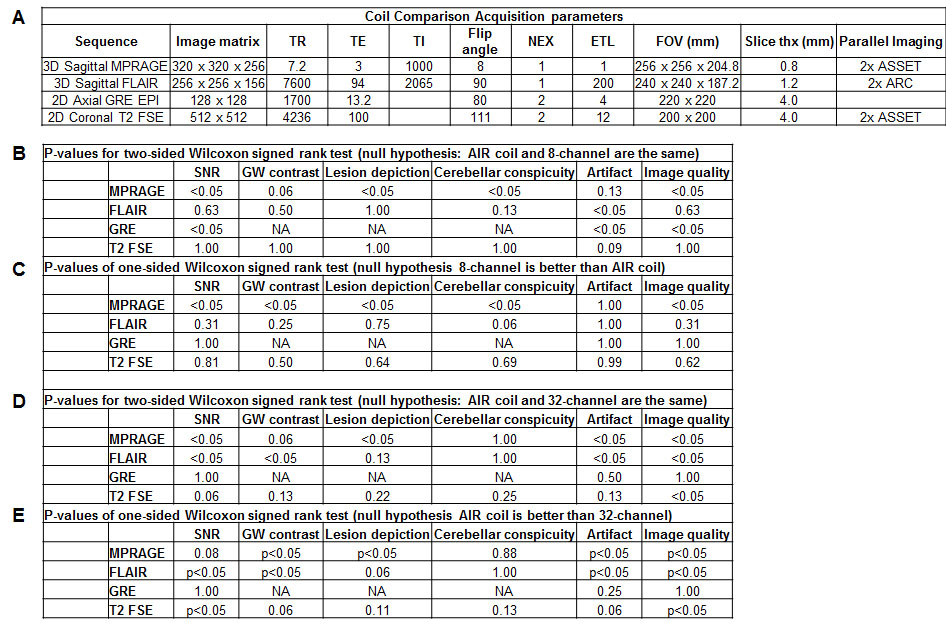
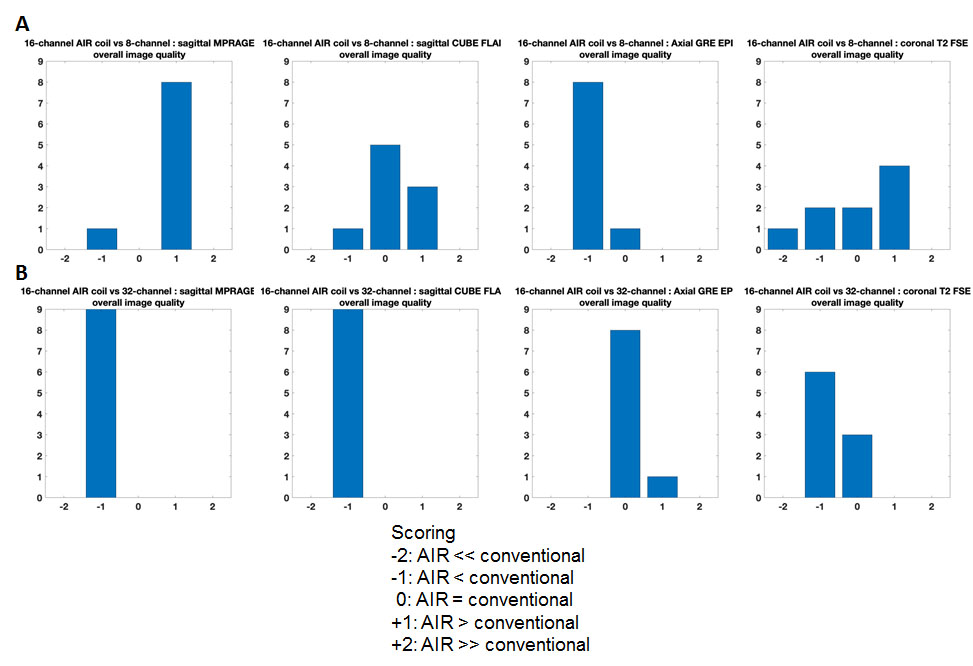
The head AIR coil is a prototype array composed of 16 overlapping circular elements sutured to a flexible, fabric balaclava ski mask (Figure 1). The 8-channel (In-vivo, Gainesville, FL) and 32-channel head coils (Nova Medical, Wilmington, MA) were used for comparison. Under an IRB-approved protocol and following written informed consent, nine healthy volunteers were imaged. Imaging experiments were performed on a high-performance C3T system (3) utilizing the following pulse sequences: sagittal MPRAGE, sagittal T2 FLAIR, axial GRE EPI, and coronal T2 FSE (Figure 2). Two board-certified neuroradiologists in consensus graded the AIR coil against each the 8-channel and 32-channel coil on a five-point ordinal scale from +2 to -2 with +2 indicting strong preference for the AIR coil and -2 indicating a strong preference for the 8/32 channel coil. The categories scored included signal-to-noise ratio, gray-white matter contrast, lesion depiction, cerebellar folia conspicuity, artifact, and overall image quality. Statistical analysis was performed using one and two-sided Wilcoxon signed rank tests.Results
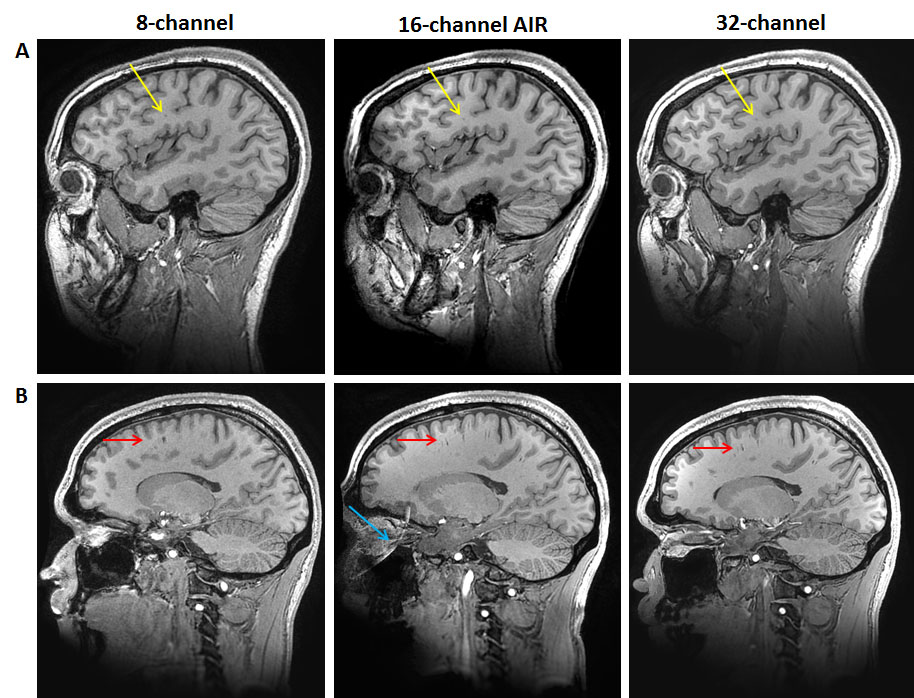
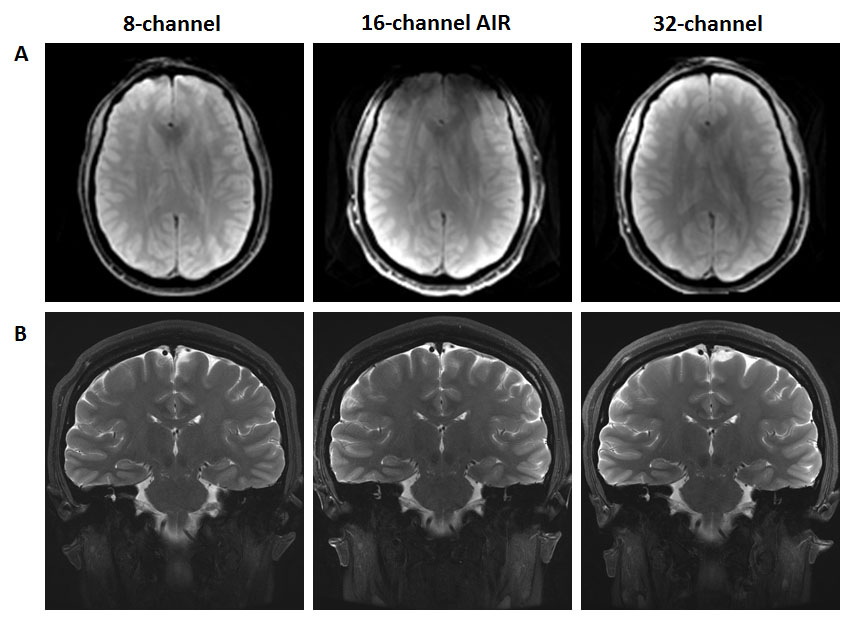
Representative images are shown in Figures 3 and 4. Figures 2 and 5 summarize the results from the image review. The AIR coil showed improved SNR, lesion depiction, cerebellar conspicuity, and overall image quality on the MPRAGE acquisition compared to the 8-channel coil. The 8-channel coil performed better on the GRE sequence across all categories, and across all sequences showed better signal uniformity and less artifact. The two coils otherwise performed similarly on the T2 FLAIR and T2 FSE sequences. Compared to the 32-channel coil, the AIR coil showed lower overall image quality on the MPRAGE, T2 FLAIR, and T2 FSE sequences, primarily driven by lower SNR and more artifacts, but performed similarly on the GRE. The primary artifacts with the 16-channel coil were ghosting and motion.Discussion
Overall, the 16-channel AIR coil performed similar to slightly better than the conventional 8-channel coil, though not as well as the 32-channel coil. A primary drawback of the 16-channel coil was the presence of motion induced artifact as the subject’s head could not be as well stabilized in the coil (Figure 1). In future prototypes the coil elements may be better protected to allow for a more secure positioning and therefore reducing the motion artifact. Differences in SNR, gray-white matter contrast, and lesion depiction between coils (8-channel < 16-channel AIR < 32-channel) were most noticeable on the MPRAGE sequence, which has the highest spatial resolution of the tested sequences. This suggests that the AIR coil may perform well relative to conventional 8-channel head coils in advanced image techniques that push the spatial resolution and SNR limits. However, the current design does not perform as well as the 32-channel coil. The 8-channel coil performed better on the low spatial resolution GRE sequence, due to better uniformity and less artifact. Though not specifically scored, image uniformity was best for the 8-channel coil across all sequences, whereas the 16-channel AIR and 32-channel coils showed relatively increased signal peripherally, as expected for close fitting arrays with smaller coil elements.Conclusion
On average the novel 16-channel head AIR coil with an open, ski-mask design performs comparable to a conventional 8-channel head coil, though not as well as a conventional 32-channel coil on standard clinical sequences. This study demonstrates feasibility of AIR coil technology for imaging of the brain and provides insight for future coil design improvements. Advantages of the AIR coil technology may be better realized with future designs that include more coil elements, testing of higher parallel imaging factors, use in anesthesia cases or task-based fMRI, and imaging of larger patients in which the flexible coil may offer improved fit and comfort.Acknowledgements
This work was supported in part by NIH grant U01 EB024450.References
1. Rossman P, Stormont RS, Lindsay SA, Robb F, Savitskij D, Stanley D, Huston J, Kaufmann T and McGee KP. Characterization of a new ultra-flexible, low profile RF receive coil technology. Int. Society of Magnetic Resonance in Medicine 25th Annual Meeting & Exhibition, Honolulu, HI. 2017; 76.
2. McGee KP, Stormont RS, Lindsay SA, Taracila V, Savitskij D, Robb F, Witte RJ, Kaufmann TJ, Huston J, Riederer SJ, Borisch EA and Rossman PJ. Characterization and evaluation of a flexible MRI receive coil array for radiation therapy MR treatment planning using highly decoupled RF circuits. Phys Med Biol 2018; 63.
3. Foo TK, Laskaris E, Vermilyea M, Xu M, Thompson P, Conte G, Van Epps C, Immer C, Lee SK, Tan ET, Graziani D, Matheiu JB, Hardy CJ, Schenck JF, Fiveland E, Stautner W, Ricci J, Peil J, Park K, Hua Y, Bai Y, Kagan A, Stanley D, Weavers PT, Gray E, Shu Y, Frick MA, Campeau NG, Trzasko J, Huston J, Bernstein MA. Lightweight, compact, and high-performance 3T MR system for imaging the brain and extremities. Magn Reson Med 2018;1-14.
4. Weavers PT, Shu Y, Tao S, Huston J 3rd, Lee SK, Graziani D, Mathieu JB, Trzasko JD, Foo TK, Bernstein MA. Compact three-tesla magnetic resonance imager with high-performance gradients passes ACR image quality and acoustic noise tests. Med Phys. 2016; 43:1259-64.
5. Tan ET, Lee SK, Weavers PT, Graziani D, Piel JE, Shu Y, Huston J 3rd, Bernstein MA, Foo TK. High slew-rate head-only gradient for improving distortion in echo planar imaging: Preliminary experience. J Magn Reson Imaging. 2016; 44:653-64.
Figures