2965
The Use of PC Cine MRI for the Evaluation of Treatment Efficacy of ETV in Patients with Obstructive HydrocephalusDeying Wen1, Xiaoyue Zhou2, and Jiayu Sun1
1Radiology Department, West China Hospital, Sichuan, China, Cheng du, Sichuan, China, China, 2MR Collaboration, Siemens Healthcare Ltd., Shanghai, China, Shanghai, China, China
Synopsis
Phase contrast cine MRI technology can help us understand the pathogenesis of diseases impacting the cerebral ventricular system by quantitatively analyzing intracranial flow of blood and cerebrospinal fluid and can provide a basis for research on new clinical treatments on these diseases. In this study, the non-invasive phase contrast cine MRI technique was used to quantitatively analyze the circulatory dynamics of cerebrospinal fluid and cerebral blood flow in patients with obstructive hydrocephalus. Early postoperative prognosis indicators were determined by comparing patients with healthy controls and by comparing pre- and post-operative results within the patient group.
Introduction
Obstructive hydrocephalus is a common neurosurgical disease 1-2,5, which is characterized by excessive accumulation of cerebrospinal fluid (CSF), the CSF circulation and circulatory dynamics still considered to be a "black box" and is not well described in international neurosurgery.Endoscopic third ventriculostomy (ETV) has been widely used as treatment4 ,but there are no preoperative application indications for ETV or early indicators for evaluating the efficacy of ETV quantitatively. Previous research has used PC cine MRI 1-6 to evaluate flow patterns in the cerebral aqueduct. This present study uses PC cine MRI to identify preoperative application indications and early indicators of the efficacy of ETV.Methods
A total of 60 neurosurgical inpatients (35 males, 25 females, mean age of 14.2 years) with obstructive hydrocephalus and 30 healthy volunteers (15 males, 15 females, mean age of 15.8 years) were enrolled from June 2017 to June 2018. Inpatients and volunteers were divided into three groups by their age: group 1, ≤ 6 years (20 inpatients); group 2 ,between 7-13 years (20 inpatients); group 3, ≥ 14 years (20 inpatients). Informed consent was obtained from all subjects. A routine MR scan of the brain was performed and included pulse-gated monitoring of multi-site PC cine MRI sequence.Patients underwent the scan twice (i.e. pre- and post-operatively). A 3T MR scanner (MAGNETOM Skyra, Siemens Healthcare, Erlangen, Germany) with a 16-channel head coil was used for all MR scans. Six anatomic locations were monitored using the PC cine MRI: the cerebral aqueduct, the fourth ventricle, the fourth ventricle outflow tract, the prepontine cistern, the foramen magnum, and the fistula of the third ventriculostomy (Fig 1). Qualitative evaluation of the CSF flow was made by two experienced radiologists independently. Regions of interest (ROI) were placed on the 6 aforementioned anatomic locations within a cardiac cycle (Fig 2). Dedicated image post-processing software (Singo via-single sign, Siemens Healthcare, Erlangen, Germany) was then used to analyze dynamic indicators, including peak velocity, mean flow velocity, average flow rate, pressure gradient, and flow pattern. Paired t-tests were used to compare the different predictors pre- and post-operatively within the same age groups. T-tests were also used to compare the indicators between patients in both their pre- and post-operative state and healthy controls.Results
We found on the preoperative imaging that the waveform, representing CSF flow, was irregular, indicating decreased or non-existent flow, at all selected anatomic locations (Fig 3,A,B). The CSF flow in the fistula of the third ventriculostomy on post-operative imaging was unobstructed and presented bidirectional pulsatile waves (Fig 3,C,D), that were similar to the cerebral aqueduct waves of the healthy controls. The mean flow velocity and average flow rate in the fistula area were significantly higher than those in the cerebral aqueduct area (P <0.05). Parameters of the prepontine cistern on postoperative imaging were higher than those on pre-operative imaging (P <0.05)and presented bidirectional pulsatile waves. There was no significant difference in the dynamic parameters at all the anatomic locations between patients in their post-operative state and the healthy controls (P> 0.05).Discussion
Preoperative cerebrospinal fluid is partially or completely blocked in patients with obstructive hydrocephalus,by monitoring the cerebrospinal fluid flow at multiple sites by PC cine MRI,and combined with clinical surgical indications of ETV, to find a suitable preoperative quantitative index for ETV.Postoperative imaging showed that the cerebrospinal fluid resumed flow through the bottom of the third ventricle and that the dynamic index of the ventral side of the brainstem increased to some extent. Furthermore, all dynamic indicators at all the anatomic locations changed significantly before and after surgery. Further research will be needed to determine whether these indicators can be used to evaluate postoperative efficacy. The main limitations of this study are its short duration and limited sample size.Conclusion
PC cine MRI reliably allows for the qualitative and quantitative analysis of changes in CSF dynamics and provides an objective basis for assessing the efficacy of ETV.Acknowledgements
No acknowledgement found.References
1.Bezuidenhout AF, Kasper EM, Baledent O, Rojas R, Bhadelia RA (2018) Relationship between pineal cyst size and aqueductal CSF flow measured by phase contrast MRI. Journal of neurosurgical sciences.2.ElSankari S, Baledent O, van Pesch V, Sindic C, de Broqueville Q, Duprez T (2013) Concomitant analysis of arterial, venous, and CSF flows using phase-contrast MRI: a quantitative comparison between MS patients and healthy controls. Journal of cerebral blood flow and metabolism : official journal of the International Society of Cerebral Blood Flow and Metabolism 33:1314-1321.3.Frolov S, Prothmann S, Liepsch D, Balasso A, Berg P, Kaczmarz S, Kirschke JS, Ichikawa S, Motosugi U, Okumura A, Shimizu T, Onishi H (2017) Measurement of Cerebrospinal Fluid Flow Dynamics Using Phase Contrast MR Imaging with Bilateral Jugular Vein Compression: A Feasibility Study in Healthy Volunteers. PloS one.4.Kulkarni AV, Drake JM, Mallucci CL, Sgouros S, Roth J, Constantini S (2009) Endoscopic third ventriculostomy in the treatment of childhood hydrocephalus. The Journal of pediatrics 155:254-259.e251.5.Peng SL, Su P, Wang FN, Cao Y, Zhang R, Lu H, Liu P (2015) Optimization of phase-contrast MRI for the quantification of whole-brain cerebral blood flow. Journal of magnetic resonance imaging : JMRI 42:1126-1133.6.Hamilton R, Baldwin K, Fuller J, Vespa P, Hu X, Bergsneider M (2012) Intracranial pressure pulse waveform correlates with aqueductal cerebrospinal fluid stroke volume. Journal of applied physiology (Bethesda, Md. : 1985) 113:1560-1566.Figures
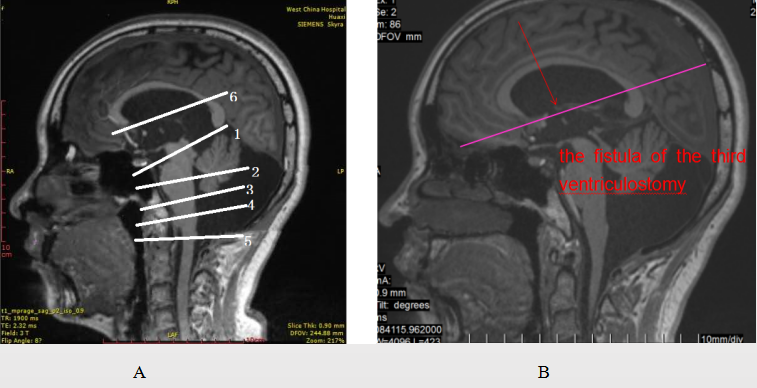
Figure1:AThe six anatomic regions of interest:1-the cerebral aqueduct, 2-fourth ventricle, 3-prepontine cistern, 4-fourth ventricle outflow tract, 5-foramen magnum, 6-The fistula of the third ventriculostomy. Each scan level is perpendicular to the corresponding anatomic location. B, The exact location of the fistula of the third ventriculostomy.
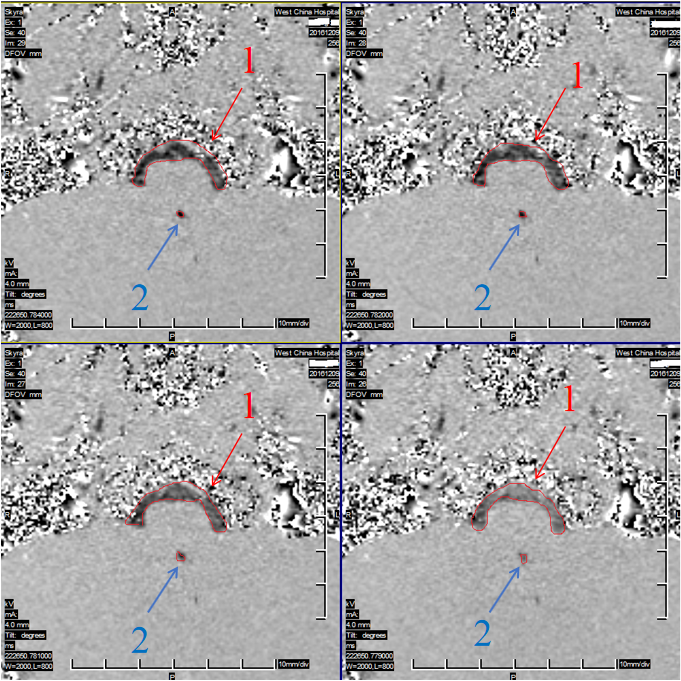
Figure2:Regions of interest (ROI) were placed on the 6 aforementioned anatomic locations within a cardiac cycle .Sketch the correct ROI area manually based on location and size of ROI.ROIs at different phases of the PC cine sequence. 1,The ROI of prepontine cistern. 2, The ROI of cerebral aqueduct.
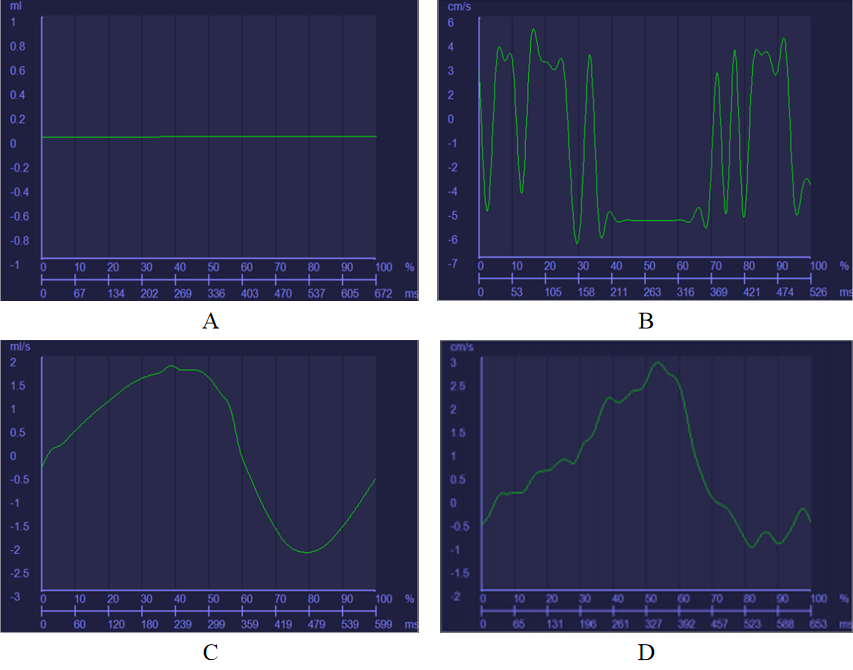
Figure3: A, The decreased to non-existent pre-operative CSF flow pattern. B, Pre-operative irregular waveform. C, Sinusoidal post-operative flow pattern.D,Post-operative flow pattern displaying an inverted "U" shape. Both post-operative waveforms were bidirectional pulsatile after being irregular before ETV.