2963
Changes in Cerebellar and Brainstem Tissue Motion in Chiari Malformation Type I Patients Following Posterior Fossa Decompression Surgery1Conquer Chiari Research Center, Department of Biomedical Engineering, The University of Akron, Akron, OH, United States, 2Laboratory of FMRI Technology (LOFT), USC Stevens Neuroimaging and Informatics Institute, Keck School of Medicine, University of Southern California, Los Angeles, CA, United States, 3Department of Neurosurgery, Emory University, Atlanta, GA, United States, 4Department of Radiology & Imaging Sciences and Biomedical Engineering, Emory University, Atlanta, GA, United States
Synopsis
Chiari type I malformation (CMI) patients have altered brain morphology and tissue motion compared to healthy controls. This motion may be the underlying cause of Chiari symptoms, such as occipital headaches. Highly symptomatic patients may be treated with posterior fossa decompression (PFD) surgery to restore cerebrospinal fluid flow and relieve brainstem compression. To quantitatively assess changes in brain tissue motion before and after surgery, we examined brainstem and cerebellar tissue displacement before and after surgery in 10 patients using spiral cine DENSE MRI. We found that tissue displacement in these structures in CMI patients is significantly reduced by PFD surgery.
Introduction
Patients with Chiari malformation type I (CMI) have altered morphology and brain tissue motion compared to healthy individuals (1-3). These motion alterations may be the underlying cause of symptoms due to repeated compression of the cerebellum, brainstem, and upper cervical cord; however, this remains unproven. Highly symptomatic CMI patients are often treated surgically with posterior fossa decompression (PFD) surgery. The goal of this surgery is to restore cerebrospinal fluid flow and relieve brainstem compression by altering cranio-cervical morphology (4). While most CMI patients have reported improvement in symptoms following PFD surgery, improvement is not consistent across all symptoms or all subjects, and selection of candidates for surgery is currently based on subjective symptomology (5). Thus, selection of surgical candidates may benefit from the ability to quantitatively assess brain tissue motion. Brain tissue motion before and after PFD surgery has been previously quantified at a select number of landmarks within the cerebellum and brainstem (3). However, tissue displacement over the entirety of these structures has not been assessed. We have previously used displacement encoding with stimulated echoes (DENSE) MRI to quantify sub-pixel levels of brain tissue displacement in healthy subjects (6). In the current study, we acquired DENSE images to determine tissue displacement before and after PFD surgery in CMI patients. We hypothesized that motion within the cerebellum and brainstem will significantly decrease following PFD surgery.Methods
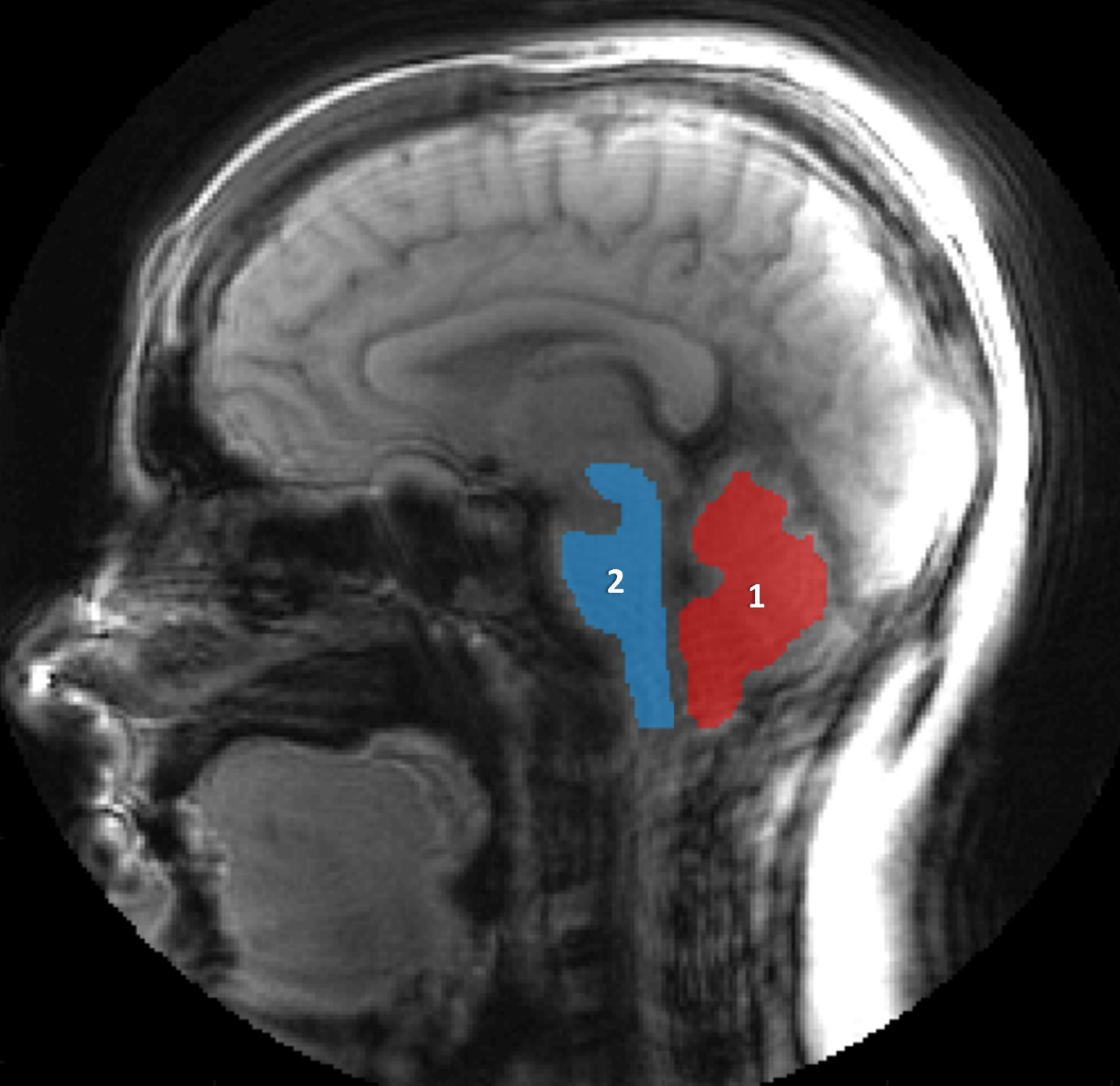
Ten CMI participants (9 females, age 35 ± 6) were imaged before and after PFD surgery in an IRB-approved study. CMI diagnosis was determined through presence of a greater than 5 mm tonsillar descent below the foramen magnum using a previous clinically-based imaging study in addition to the presence of clinical symptoms. All patients had PFD surgery and were referred by a single neurosurgeon (DB). The study protocol included a cardiac-gated, spiral cine DENSE sequence performed at the mid-sagittal plane on a 3T MRI scanner (Siemens Prisma, Erlangen, Germany). Acquisition parameters included: two directions of in-plane motion encoding, encoding frequency of 0.6 cycles/mm, two spiral interleaves per heartbeat, pixel size of 1.2 × 1.2 mm2, slice thickness of 7 mm, four signal averages, 16-27 frames over the cardiac cycle, depending on the heart rate. A MATLAB (Mathworks, Natick, MA) based program (DENSEpro) was developed to evaluate tissue motion from the DENSE phase images. Using DENSEpro, two regions (brainstem and cerebellum, Fig. 1) were manually segmented on midsagittal DENSE magnitude images before and after surgery in all subjects by a single observer (ME). The pixel-by-pixel displacement magnitudes over the cardiac cycle were used to determine maximal tissue displacement, which was calculated for each pixel and displayed as a displacement colormap. These maximal tissue displacement values were then spatially averaged for the brainstem and cerebellum in each subject (referred to as mean maximum displacement). Differences in spatially averaged maximal tissue motion before and after surgery were determined using paired sample t-tests, and statistical significant was evaluated as p < 0.05.
Results
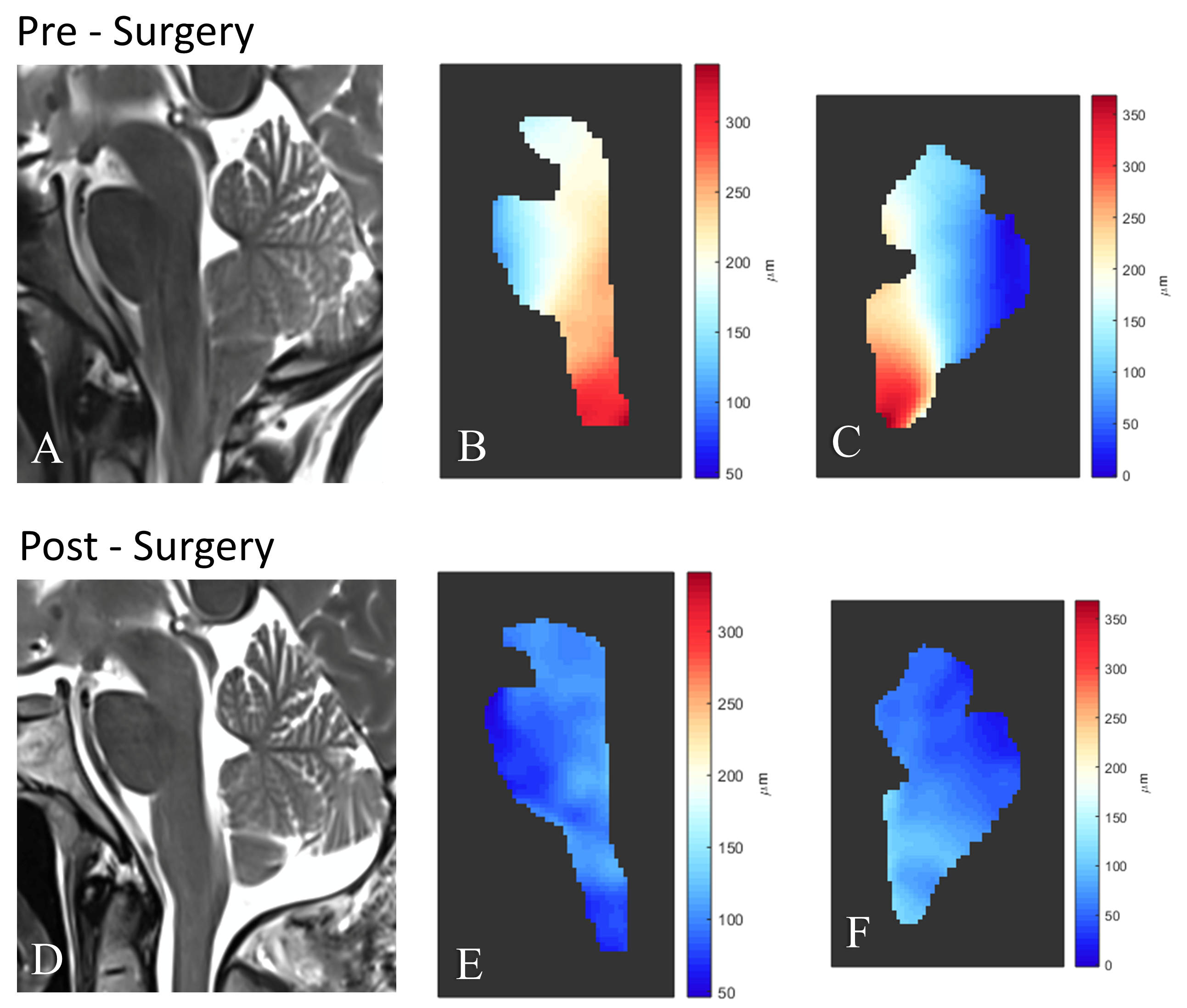
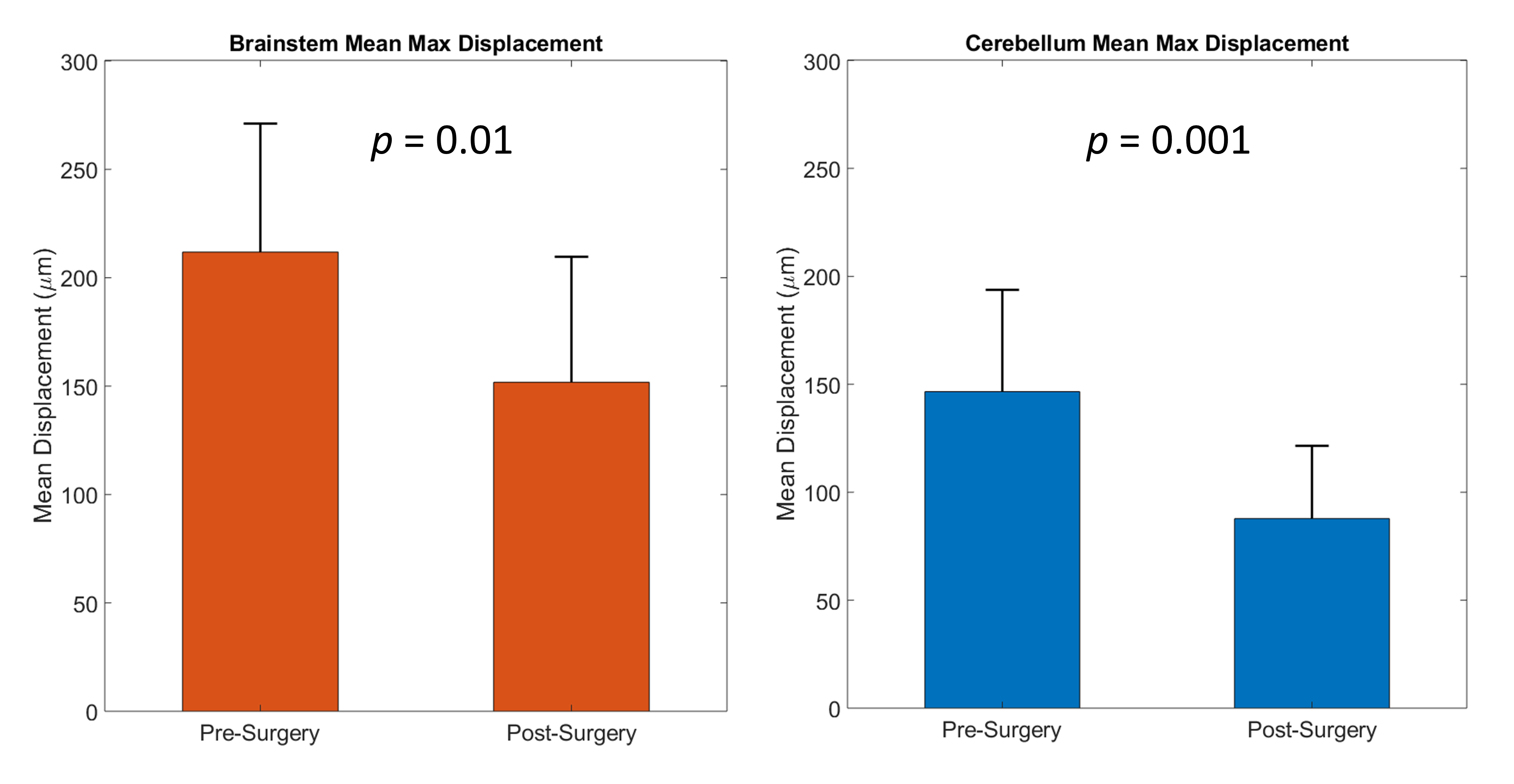
All 10 subjects completed the pre- and post-surgery imaging protocol, and the displacement maps and spatially-averaged values of maximal displacement were determined. An example of pre- and post-surgery displacement map for one subject is shown in Figure 2 and illustrates the substantial reduction of displacement in the inferior cerebellum and brainstem. Spatially-averaged (mean) values of maximum tissue displacement in the cerebellum decreased 40% following PFD surgery (mean ± SD: -59 ± 39 μm, p = 0.001, Figure 3). Maximum displacement within the brainstem was reduced by 28% following PFD surgery (-60 ± 62 μm, p = 0.01, Figure 3). This reduction primarily occurred in the craniocaudal direction.Discussion
The major finding of this study is that spiral cine DENSE imaging was able to show that PFD surgery results in a significant reduction in cardiac induced displacement of the cerebellum and brainstem of patients with CMI. For the first time, quantitative measurements of brain parenchyma displacement on a pixel by pixel basis that is affected by PFD surgery were obtained in this study. This finding is noteworthy as this sub-occipital region is often cited by Chiari patients as a region of pain that often resolves with surgery. Further studies will examine temporal characteristics of motion, motion in other brain regions, and calculation of tissue strain.Conclusion
We have shown that tissue displacement in the cerebellum and brainstem is significantly reduced by PFD surgery. The use of cardiac-gated spiral cine DENSE imaging enables sub-pixel measurements of displacement.Acknowledgements
This work was funded by a Grant from Conquer Chiari.References
- Hofmann E, Warmuth-Metz M, Bendszus M, Solymosi L. Phase-contrast MR imaging of the cervical CSF and spinal cord: volumetric motion analysis in patients with Chiari I malformation. American Journal of Neuroradiology. 2000;21(1):151-8.
- Houston JR, Eppelheimer MS, Pahlavian SH, Biswas D, Urbizu A, Martin BA, Bapuraj JR, Luciano M, Allen PA, Loth F. A morphometric assessment of type I Chiari malformation above the McRae line: A retrospective case-control study in 302 adult female subjects. Journal of Neuroradiology. 2017.
- Leung V, Magnussen JS, Stoodley MA, Bilston LE. Cerebellar and hindbrain motion in Chiari malformation with and without syringomyelia. Journal of Neurosurgery: Spine. 2016;24(4):546-55.
- Yilmaz A, Kanat A, Musluman AM, Colak I, Terzi Y, Kayaci S, Aydin Y. When is duraplasty required in the surgical treatment of Chiari malformation type I based on tonsillar descending grading scale? World Neurosurg. 2011;75(2):307-13. doi: 10.1016/j.wneu.2010.09.005. PubMed PMID: 21492735.
- Giammattei L, Messerer M, Daniel R, Aghakhani N, Parker F. Long term outcome of surgical treatment of Chiari Malformation without syringomyelia. Journal of neurosurgical sciences. 2017.
- Pahlavian S, Oshinski J, Zhong X, Loth F, Amini R. Regional Quantification of Brain Tissue Strain Using Displacement-Encoding With Stimulated Echoes Magnetic Resonance Imaging. Journal of biomechanical engineering. 2018;140(8).
Figures