2962
Isointense Clot Sign as a Predictor of Complete Recanalization in Patients with Cerebral Venous Sinus Thrombosis1Radiology, Xuanwu Hospital, Capital Medical University, Beijing, China, 2Emergency, Xuanwu Hospital, Capital Medical University, Beijing, China, 3Neurology, Xuanwu Hospital, Capital Medical University, Beijing, China, 4Neurosurgery, Xuanwu Hospital, Capital Medical University, Beijing, China, 5Radiology, Biomedical Imaging Research Institute, Cedars Sinai Medical Center, Los Angeles, CA, United States, 6Neurology, Department of Neurology, Beth Israel Deaconess Medical Center, Boston, Malaysia
Synopsis
This
study aims to investigate the association of thrombus characteristics with
complete recanalization in cerebral venous sinus thrombosis (CVST) patients
undergoing endovascular treatment using Magnetic Resonance Black-blood Thrombus
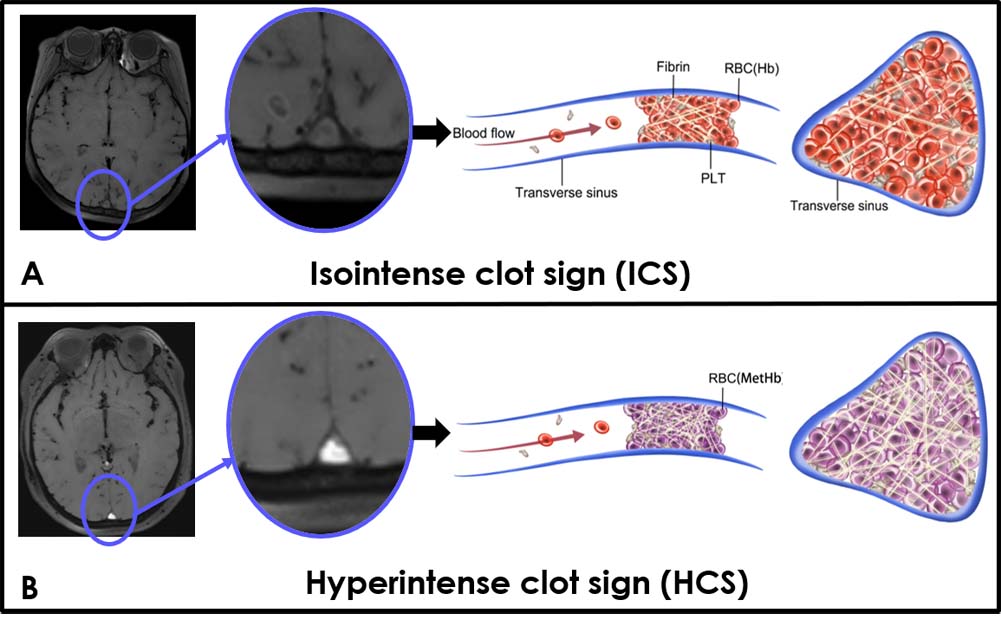
Imaging (MRBTI). There was more detection of isointense clot sign (ICS) in
complete recanalization group than partial recanalization group. Logistic
regression analysis showed that ICS was associated with complete recanalization,
which means ICS on MRBTI can be a predictor of complete recanalization in CVST
patients having endovascular treatment. So, we think that MRBTI will improve
efficacy of endovascular therapy and help eliminate adverse outcomes.
Introduction
Cerebral venous sinus thrombosis (CVST) is a relatively uncommon cause of stroke with various symptoms [1]. Systemic anticoagulation has been regarded as the first-line treatment for CVST [2]. However, anticoagulation alone does not always dissolve large and extensive CVST [3]. Endovascular intervention is an alternative option for patients who deteriorate despite the use of anticoagulation [4]. Since the thrombus itself is the primary target of endovascular therapy, understanding its composition is essential for complete resolution of the clot. CT and MR Venography are indirect luminal imaging methods based on venous flow perturbation caused by thrombi, and these techniques cannot stage and quantify the thrombus. Magnetic resonance black-blood thrombus imaging (MRBTI) has recently been proposed as a non-invasive imaging tool for the direct thrombus imaging [5]. The purpose of this study was to evaluate thrombus characteristics affecting the extent of recanalization in patients with CVST undergoing endovascular therapy.Methods
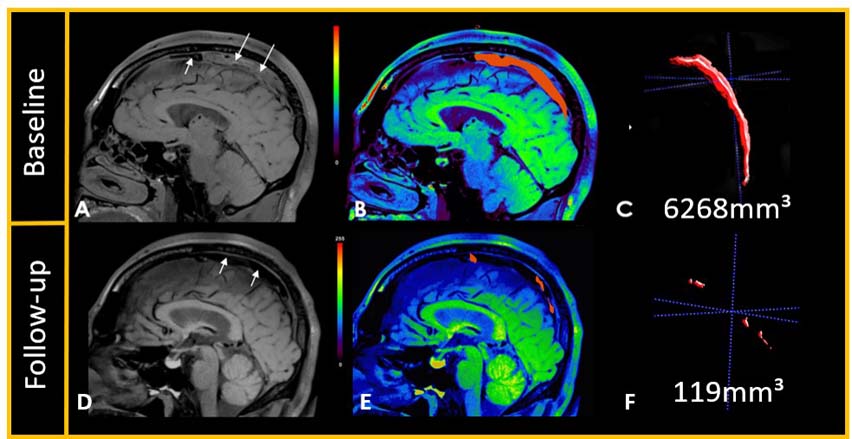
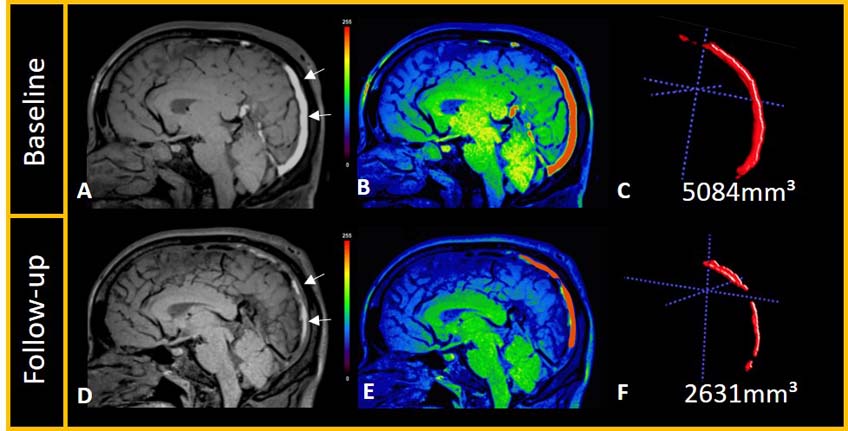
Acute and subacute CVST patients scheduled for endovascular treatment were prospectively recruited into our study. MR data was collected on a MAGNETOM Verio 3T MR scanner (Siemens Healthcare, Erlangen, Germany) with a 32-channel head coil. Each thrombosed venous segment was evaluated regarding complete or partial recanalization based on digital subtraction angiography (DSA) after treatment. MRBTI was performed before and after the endovascular treatment. The 14 venous segments were included. The signal to noise ratio (SNR) of the clot, age of the clot and baseline volume of the clot were compared between the complete and partial recanalization groups. A logistic regression analysis was performed to identify the association between these clot characteristics and recanalization status.Results
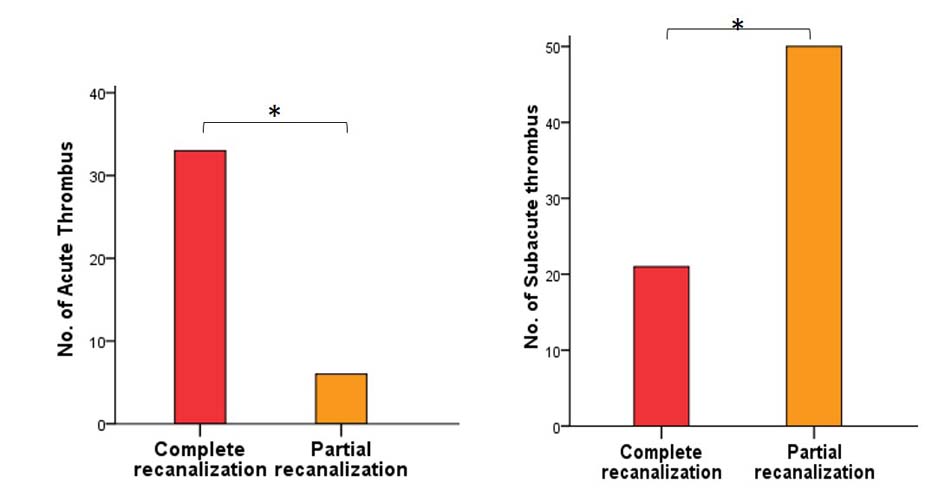
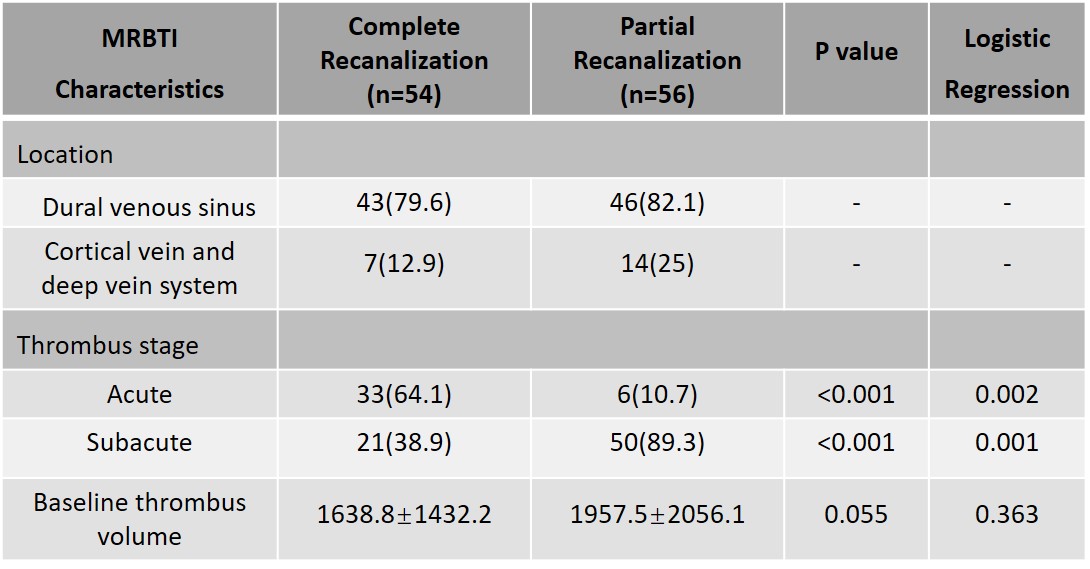
Twenty-one CVST patients (12 female, age 32.5±9.8) undergoing endovascular therapy were prospectively included. 110 thrombosed segments were identified on DSA. Complete recanalization occurred in 54 segments and partial recanalization in 56 segments after endovascular treatment. There was a significant difference in the SNR of CVST clot between the complete and partial recanalization groups (120.5±47.2 vs 169.3±80.5, P<0.001). An isointense clot sign (ICS) was found in 39 segments and a hyperintense clot sign (HCS) was found in 71 segments. Logistic regression analysis showed that ICS on MRBTI was associated with complete recanalization (P<0.001, odds ratio=3.937, 95% confidence interval, 1.6-9.5). There was no significant difference on baseline volume of the clot (1638.8±1432.2 mm3 vs 1957.5±2056.1 mm3, P>0.05) between the complete and partial recanalization groups. The baseline volume of thrombus was not associated with complete recanalization (P=0.363).Discussion
This study showed that ICS was independently associated with complete recanalization. We found that acute clot was easier to recanalize compared with subacute clot. This is the first study investigating the association between clot age and recanalization of thrombosed segments in patients undergoing endovascular therapy for CVST.
Endovascular treatment can be considered as an alternative therapeutic option in patients with worsening symptoms CVST [6]. Selection of an effective therapy depends on many factors including the accurate determination of thrombus age and maturity [7]. Thus, there is a growing need to develop better novel minimally invasive imaging techniques and diagnostic tools to accurately determine clot age in CVST. Hemoglobin in the thrombus changes from deoxyhemoglobin to methemoglobin in parallel to the duration of symptoms which can be used as imaging target. MRBTI with hyper T1 weighting can differentiate acute (ICS) and sub-acute (HCS) thrombus based on their intrinsic MR signal intensity characteristics.
Thrombus composition is a factor in determining susceptibility to mechanical clot disruption and thus the degree of successful recanalization. Understanding the age of the thrombus can help to determine the benefits and risks of treatment, as well as the likelihood of treatment success. Acute clot is easier to completely recanalize because it primarily consists of red blood cells. When acute thrombi age, they become mechanically less compliant due to fibrin cross linking and collagen deposition over time. Sub-acute thrombi, which are rich in collagen and cross-linked fibrin, harden and are more difficult to disrupt.
There were several limitations in the current study. First, the present study was performed on a limited number of CVST patients who underwent endovascular therapy. Second, our classification of clot types is imperfect because precise interpretation of thrombus composition may need multi contrast MR sequences which were not performed in the current study. Finally, we didn’t perform pathology on the retrieved clots.
Conclusion
ICS on MRBTI can be used to predict complete recanalization in patients receiving endovascular treatment. MRBTI provides a robust method to define clot composition, and is potentially useful in selecting the most appropriate CVT patients for endovascular treatment.Acknowledgements
The authors thank all the participants who gave their time to the study.References
1. Silvis SM. de Sousa DA, Ferro JM, Coutinho JM. Cerebral venous thrombosis. Nat Rev Neurol. 2017;13: 555-565. 2. Ferro JM, Bousser MG, Canhao P, Coutinho JM, Crassard I, Dentali F, et al. European Stroke Organization guideline for the diagnosis and treatment of cerebral venous thrombosis-endorsed by the European Academy of Neurology. Eur J Neurol. 2017;24: 1203-1213. 3. Capecchi M, Abbattista M., Martinelli, I. Cerebral venous sinus thrombosis. J Thromb Haemost. 2018;16:1918-1931. 4. Einhaupl K, Stam J, Bousser MG, De Bruijn SF, Ferro JM, Martinelli I, et al. EFNS guideline on the treatment of cerebral venous and sinus thrombosis in adult patients. Eur J Neurol. 2010;17:1229-1235. 5. Yang Q, Duan J, Fan Z, Qu X, Xie Y, Nguyen C, et al. Early Detection and Quantification of Cerebral Venous Thrombosis by Magnetic Resonance Black-Blood Thrombus Imaging. Stroke. 2016;47: 404-409. 6. Konakondla S, Schirmer CM, Li F, Geng X, Ding Y. New Developments in the Pathophysiology, Workup, and Diagnosis of Dural Venous Sinus Thrombosis (DVST) and a Systematic Review of Endovascular Treatments. Aging Dis. 2017;8:136-148. 7. Guo XB, Song LJ, Guan S. Endovascular treatment of chronic, recurrent headache secondary to chronic cerebral venous sinus thrombosis. J Stroke Cerebrovasc Dis. 2014;23:560-563.Figures