2960
Diagnostic Image Quality and Time reduction Using Compressed SENSE with 3D NerveVIEW for MR Neurography1Philips Healthcare, Gainesville, FL, United States, 2Radiology, University of Texas Southwestern Medical Center, Dallas, TX, United States, 3Advanced Imaging Research Center, University of Texas Southwestern Medical Center, Dallas, TX, United States
Synopsis
Magnetic resonance imaging of nerves, also known as MR neurography (MRN) is an emerging technique used to assess peripheral neuropathies. 3D NerveVIEW is a heavily T2-weighted 3D acquisition that has been developed to address common challenges when scanning brachial and lumbosacral plexuses. However, 3D NerveVIEW suffers from long acquisition times. Therefore, in this study we acquired 3D NerveVIEW with compressed SENSE to accelerate scan times and assessed images for motion and pulsation artefacts, nerve signal-to-noise ratio, contrast-to-noise ratio, and nerve signal-to-fat signal ratio. 3D NerveVIEW with compressed SENSE leads to significant time savings without significant changes in image quality.
INTRODUCTION:
Magnetic resonance imaging of nerves, also known as MR neurography (MRN) is used to assess and characterize peripheral neuropathies. 3D NerveVIEW is a heavily T2-weighted 3D acquisition that has been developed to address common challenges when scanning brachial and lumbosacral plexuses where inhomogeneous fat suppression and signal from flow-related artifacts can obscure the nerve structures. 3D NerveVIEW of the brachial plexus uses a broadband adiabatic short tau inversion recovery (STIR) inversion pulse to improve fat suppression over the imaging volume. In contrast, 3D NerveVIEW of the lumbosacral plexus utilizes a spectral adiabatic inversion recovery pulse (SPAIR) to achieve fat suppression. In addition, a motion sensitized driven equilibrium (MSDE) preparation helps reduce the signal from blood in the neurovascular bundle. Although this technique has great application in MRN, it is hindered by long scan times which make its clinical feasibility and adoption problematic. These long scan times render 3D NerveVIEW an ideal candidate for applying accelerated scanning techniques, like compressed SENSE (give ref to the White paper or similar). We aimed to evaluate the image quality of the combined CS+3D NerveVIEW and plexus depiction2. Our hypothesis was that on this shorter sequence, image quality remains clinically unaffected with preserved nerve conspicuity and spatial resolution despite substantial time reduction.METHODS:
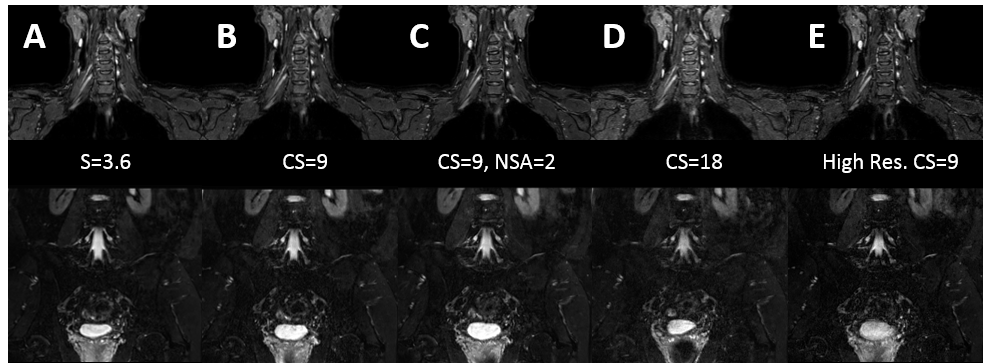
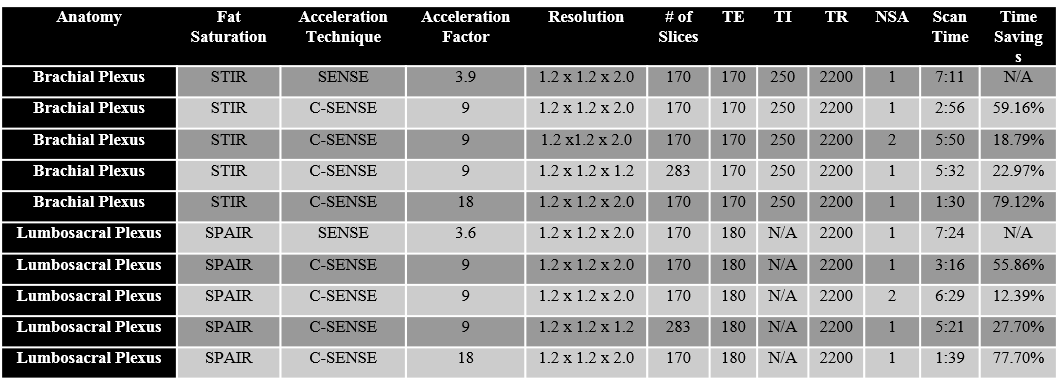
3D NerveVIEW images of the brachial (STIR) and lumbosacral plexus (SPAIR) were acquired with and without compressed SENSE (see Table 1 for image parameters) from 5 subjects on a Philips 3T Ingenia system using a combination of the 15 channel head, 16 channel anterior, and 12 channel posterior coils. Base 3D NerveVIEW images were compared to four sets of images with various factors of compressed SENSE to investigate accelerating scan times, resolution, and image quality. The images were evaluated for motion and pulsation artefacts, nerve signal-to-noise ratio (nerve signal/√air signal), contrast-to-noise ratio [(nerve signal−muscle signal)/(√air signal)], and nerve signal-to-fat signal ratio compared to the base 3D NerveVIEW sequence (see Table 1 for image parameters).RESULTS:
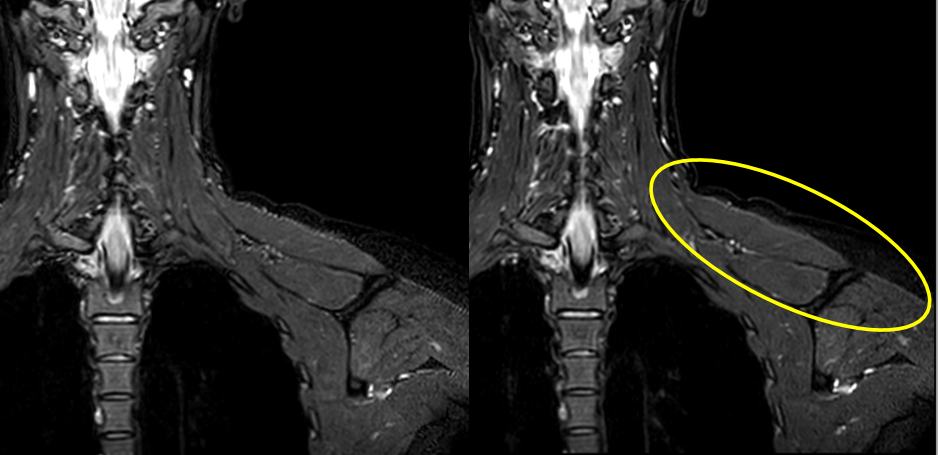
Two-tailed t-test of image quality revealed no significant differences between all the images acquired with C-SENSE compared to the base 3D NerveVIEW images with respect to the nerve signal-to-noise ratio, contrast-to-noise ratio, and nerve signal-to-fat signal ratio. All 3D NerveVIEW MRN images demonstrates homogeneous fat suppression with increased nerve signal- and contrast-to-noise ratios resulting in good nerve conspicuity of the brachial and lumbosacral plexuses (Figure 1). Image quality remained clinically unaffected while showing a scan time reduction of up to 79.12% and 77.70% for the brachial plexus and lumbar plexus respectively (Table 1). This resulted in reducing scan times for 3D NervVIEW from over seven minutes to under two minutes. In addition, using a C-SENSE acceleration of 9 with 2 signal averages resulted in reduced striation/cross-hatching artifacts from the free induction decay (Figure 2). This improvement was achieved while saving 81 seconds in the brachial plexus and 55 seconds in the lumbosacral plexus compared to the base sequence (Table 1).DISCUSSION:
MRN can significantly impact diagnostic and therapeutic outcomes in patients suffering from peripheral neuropathies and is often performed in pre-surgical planning3. 3D NerveVIEW overcomes many of the challenges when performing MRN, and has shown to be a robust and reliable technique compared to other current MRN techniques1. Techniques with long scan times, as is the 3D NerveVIEW, can lead to decreased patient comfort and the likelihood of patient motion. More importantly, long scans that have the potential to interrupt workflow and imaging efficiency thus being at risk for not being adopted clinically. Here we show three major benefits for applying C-SENSE to 3D NerveVIEW: 1) drastically shorten 3D NerveVIEW acquisition times, 2) reduce image artifacts, 3) increase spatial resolution without increasing scan times. All three benefits also preserved nerve signal-to-noise ratio, contrast-to-noise ratio, and nerve signal-to-fat signal ratio to maintain superior peripheral nerve conspicuity for MRN. Most notably application of high C-SENSE acceleration factors can provide clinically diagnostic MRN images in under two minutes.CONCLUSION:
Image quality of 3D NerveVIEW MRN with compressed SENSE is maintained while reducing scan time within a clinically acceptable range. Furthermore, the use of compressed SENSE in MRN may allow for more novel approaches to eliminate potential artifacts, improving peripheral nerve conspicuity, all the while still reducing scan time.Acknowledgements
No acknowledgement found.References
1. Kasper JM, Wadhwa V, Scott KM, Rozen S, Xi Y, Chhabra A. SHINKEI—a novel 3D isotropic MR neurography technique: technical advantages over 3DIRTSE-based imaging. European radiology. 2015;25(6):1672-7.
2. Lustig M, Donoho D, Pauly JM. Sparse MRI: The application of compressed sensing for rapid MR imaging. Magnetic Resonance in Medicine. 2007;58(6):1182-95.
3. Chhabra A, Belzberg AJ, Rosson GD, Thawait GK, Chalian M, Farahani SJ, et al. Impact of high resolution 3 tesla MR neurography (MRN) on diagnostic thinking and therapeutic patient management. European radiology. 2016;26(5):1235-44.
Figures