2959
Feasibility of brachial plexus DWI with high acceleration rate using multiband SENSE at 1.5 T1Philips Healthcare Greater China, Beijing, China, 2Philips Healthcare, Suzhou, China
Synopsis
Diffusion weighted imaging (DWI) for brachial plexus can provide valuable information for clinical practice, and the accelerated imaging techniques have been extensively evaluated. This study aims to demonstrate the DWI with high acceleration rate on brachial plexus using a multiband SENSE technique at 1.5T system.
Introduction
Diffusion weighted imaging (DWI) for brachial plexus can provide valuable information for clinical practice [1]. Simultaneous multi-slice imaging with multiband excitation and refocusing [2] is one of the state-of-the-art acceleration technologies for the acquisition and reconstruction for DWI. Multiband DWI has been extensively evaluated in the imaging for central nervous system at 3.0 T [3], but studies rarely focus on brachial plexus imaging at the lower field strength. This study aimed to demonstrate the feasibility of high acceleration rate on brachial plexus DWI using multiband SENSE (MB-SENSE) at 1.5 T.Method
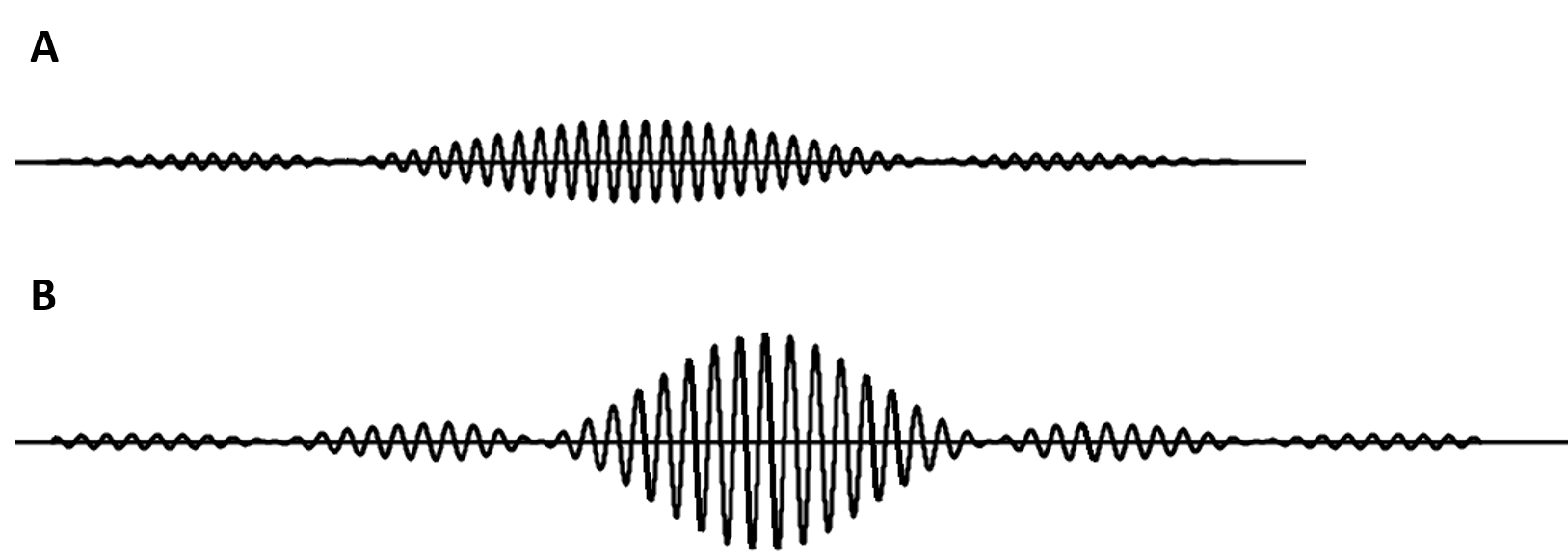
The brachial plexus diffusion imaging was performed on an Ingenia Prodiva 1.5 T MR scanner (Philips Healthcare, Suzhou, China) with healthy volunteers with informed consent, study approved by a local IRB, where a single-shot DW-EPI sequence was used. An MSK coil and a head-spine coil set were combined to cover the desired imaging FOV of 250x250 mm2. The voxel size was 3mm isotropic with TE/TR = 66/8012 ms. Traditional SENSE was applied with acceleration factor of 2 as a reference. To evaluate the feasibility of MB-SENSE with different acceleration factors, images using both MB factor = 2 and MB factor = 3 were acquired with the same SENSE factor = 2, where the kz phase encoding and coil encoding were combined to better exploit the coil sensitivities in both the phase encoding and the slice directions [4]. The excitation and the refocusing pulses for MB factor = 2 were shown in Figure 1. The duration for the excitation and refocusing pulse were 6.1 and 7.3 ms, respectively. The bandwidth for the excitation and the refocusing pulses were 663 and 598 Hz. For MB factor = 3, the durations were 9.2 and 11.0 ms for the excitation and refocusing pulses and the bandwidth were 442 and 399 Hz.Results
Figure 2 showed the brachial plexus DWI images from different acquisitions (MB turned off, MB=2, and MB=3). Images were originally acquired in the axial plane. They then went through MIP reconstruction to better display the brachial plexus in coronal plane. Compared to the reference image acquired using only an in-plane SENSE=2, the images using MB=2 showed similar image quality while the noise level was raised in the images with MB=3. Note that SENSE acceleration factor was set to 2 for both MB=2 and MB=3 acquisitions.Discussion
We demonstrated that MB-SENSE could be used to accelerate the image acquisition for brachial plexus DWI at 1.5 T. In our current study, MB=2 appeared to be an optimal choice which balanced the scan time and image quality. Using a higher MB factor may hamper the image quality, where the reduced SNR could be caused by 1) limited coil sensitivity in the phase encoding and slice directions, 2) prolonged RF pulses (both the excitation and the refocusing pulses) that led to longer TE, and 3) smaller RF bandwidth that was more prone to local B0 field inhomogeneity. The excitation and refocusing pulses were designed to possess similar bandwidth such that they can manipulate with the same slice even if it was distorted. The pulses were longer in MB=3 case than those in MB=2 case due to the B1 limit casted by the hardware, which also led to the reduced bandwidth in the MB=3 case.Conclusion
For brachial plexus DWI, image acquisition can be accelerated by combining Multiband with SENSE techniques at 1.5 T system.Acknowledgements
No acknowledgement found.References
[1] Adachi Y, et al. Brachial and lumbar plexuses in chronic inflammatory demyelinating polyradiculoneuropathy: MRI assessment including apparent diffusion coefficient. Neuroradiology 2011; 53: 3-11
[2] Barth M, et al. Simultaneous MultiSlice (SMR) imaging techniques. Magn Reson Med 2016; 75: 63-81
[3] Ugurbil K, et al. Pushing spatial and temporal resolution for functional and diffusion MRI in the Human Connectome Project. Neuroimage 2013; 80: 80-104
[4] Nunes RG, et al. Simultaneous slice excitation and reconstruction for single shot EPI. In Proceedings of the 14th Annual Meeting of ISMRM, Seattle, Washington, USA, 2006, Abstract 293
Figures