2956
Prediction of Postlaminar Optic Nerve Invasion in Retinoblastoma with MR Imaging Features1Department of Radiology, Beijing Tongren Hospital, Capital Medical University, Beijing, Beijing, China
Synopsis
Postlaminar optic nerve invasion (PLONI) is a poor prognostic indicator in retinoblastoma. However, it is not easy for both ophthalmologists and radiologists to detect it. Can the combination of conventional MR imaging findings predict PLONI ? This research devoted evidence for this question.
INTRODUCTION
Postlaminar optic nerve invasion (PLONI) is that retinoblastoma invades through the lamina cribrosa.1 The presence PLONI is a poor prognostic indicator and associated with a higher likelihood of systemic metastasis or local recurrence.2-8 Recent publications have suggested that MRI can be used to detect the presence of PLONI.9-18 Most of these studies have focused on optic nerve enhancement and the tumor size. These studies have reported relatively high specificity (84–98%), but the sensitivity was relatively low (37%-78%) with a wide range. The aim of our study was to identify additional MRI findings that improve the diagnostic performance of MRI to predict the presence of PLONI in patients with retinoblastoma.METHODS
Preoperative conventional MRI findings were evaluated in 120 eyes with retinoblastoma who underwent eyes enucleation between January 2008 and December 2017. A total of 19 MRI descriptors were assessed independently by two observers and correlated histopathologic PLONI with those MRI features. A weighted k statistic was used to assess agreement between observers. Multiple logistic regression analyses were performed to identify independent factors of PLONI. A new regression model for predicting PLONI was developed using the results of the stepwise analysis. Receiver operating characteristic curves (ROC) were used to analyze the diagnostic accuracy, and the area under the curve were calculated.RESULTS
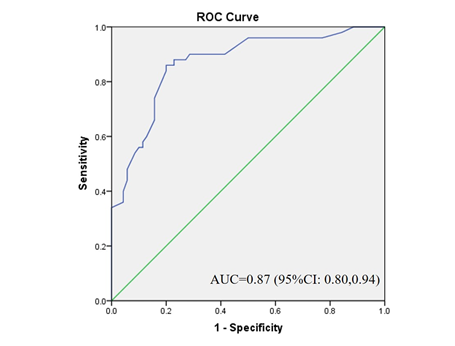
Nine MR imaging features were proved to have significant association with PLONI, including laterality(P<0.01), shape(P=0.04), diffuse infiltrating growth(P=0.04), T2 signal intensity(P=0.03), tumor site (P<0.01), optic nerve enlargement (P=0.03), optic nerve enhancement(P<0.01), crystalline lens evaluation (P=0.04), and size of the affected eye (P<0.01). The most important and significantly independent prognostic factors for PLONI were optic nerve enhancement (OR,10.52; 95%CI:3.33, 33.25), tumor totally covering the optic disk (OR, 10.75; 95%CI:1.07, 107.64), tumor located in the right side (OR, 3.46; 95%CI:1.17,10.17) or bilateral (OR, 20.35; 95%CI:2.57, 335.36), isointense on T1WI (OR, 3.96; 95%CI:1.39, 11.36) and hypointense on T2WI (OR, 0.26; 95%CI:0.09, 0.71).Receiver operating characteristic (ROC) analysis for the model with MR imaging features yielded areas under the curve of 0.87 (95% CI: 0.80-0.94, P< .0001) for PLONI (Fig.1). The sensitivity was 86% and the specificity was 80% based on the cutoff of maximum Youden index.DISCUSSION
In our study based on multivariate analysis, the ROC analysis for five MRI features yielded AUCs of 0.87 with sensitivity and specificity of 86% and 80%, respectively. Compared with previous research 9,12-16, 18, 19, we've got better predictive performance and significantly higher specificity. Logistic regression model based on MR features may have a relatively higher ability to predict the PLONI than model based on tumor sizes. Interestingly, in our study based on multivariate analysis, we found that tumors located in the right eye or bilateral were more likely to invade the postlaminar optic nerve. Although many studies suggested that there was no association between histopathologic risk factors and the laterality of RB6, 20-22, bilateral retinoblastomas were likely to have a poor prognosis and clinical outcome23, 24. In this work, the laterality of RB was associated with PLONI. This could be due to a genetic difference between these tumors, or it could simply be due to the fact that bilateral RB patients have more tumors (larger tumor volumes). In previous studies, the signal intensity of tumors was mostly compared with the vitreous body.18, 25, 26 Retinoblastoma typically demonstrates moderate hyperintensity compared to the vitreous body on T1-weighted images and moderate hypointense on T2-weighted images, with moderate to marked enhancement and reduced diffusion. In our series the T1 and T2 signal intensity of tumors were compared with gray matter. Tumors that were isointense to gray matter on T1-weighted images were more likely to invade the postlaminar optic nerve, and those showed isointense on T2-weighted images were more likely to be without postlaminar optic nerve invasion. The limitations of this study was we only evaluated some subjective features, lacking of objective quantified indicators such as diameter and volume.CONCLUSION
MR imaging features of retinoblastoma show a strong association with PLONI. The model with MR imaging features demonstrated promising prediction performance in detecting PLONI.Acknowledgements
No acknowledgement found.References
1. Chantada GL, Casco F, Fandiño AC, et al. Outcome of Patients with Retinoblastoma and Postlaminar Optic Nerve Invasion. Ophthalmology. 2007;114(11):2083-2089.
2. Khelfaoui F, Validire P, Auperin A, et al. Histopathologic risk factors in retinoblastoma: a retrospective study of 172 patients treated in a single institution. Cancer-Am Cancer Soc. 1996;77(6):1206-1213.
3. Kopelman JE, Mclean IW, Rosenberg SH. Multivariate analysis of risk factors for metastasis in retinoblastoma treated by enucleation. Ophthalmology. 1987;94(4):371-377.
4. Magramm I, Abramson DH, Ellsworth RM. Optic nerve involvement in retinoblastoma. Ophthalmology. 1989;96(2):217-222.
5. Messmer EP, Heinrich T, Höpping W, De SE, Havers W, Sauerwein W. Risk factors for metastases in patients with retinoblastoma. Ophthalmology. 1991;98(2):136-141.
6. Khelfaoui F, Validire P, Auperin A, et al. Histopathologic risk factors in retinoblastoma: a retrospective study of 172 patients treated in a single institution. Cancer-Am Cancer Soc. 1996;77(6):1206-1213.
7. Sastre X, Chantada GL, Doz F, et al. Proceedings of the consensus meetings from the International Retinoblastoma Staging Working Group on the pathology guidelines for the examination of enucleated eyes and evaluation of prognostic risk factors in retinoblastoma. Arch Pathol Lab Med. 2009;133(8):1199-1202.
8. Kaliki S, Shields CL, Rojanaporn D, et al. High-Risk Retinoblastoma Based on International Classification of Retinoblastoma: Analysis of 519 Enucleated Eyes. Ophthalmology. 2013;120(5):997-1003.
9. De Jong MC, van der Meer FJ, Goricke SL, et al. Diagnostic Accuracy of Intraocular Tumor Size Measured with MR Imaging in the Prediction of Postlaminar Optic Nerve Invasion and Massive Choroidal Invasion of Retinoblastoma. Radiology. 2016;279(3):817-826.
10. de Graaf P, Barkhof F, Moll AC, et al. Retinoblastoma: MR imaging parameters in detection of tumor extent. Radiology. 2005;235(1):197-207.
11. Brisse HJ, Guesmi M, Aerts I, et al. Relevance of CT and MRI in retinoblastoma for the diagnosis of postlaminar invasion with normal-size optic nerve: a retrospective study of 150 patients with histological comparison. Pediatr Radiol. 2007;37(7):649-656.
12. de Jong MC, de Graaf P, Noij DP, et al. Diagnostic Performance of Magnetic Resonance Imaging and Computed Tomography for Advanced Retinoblastoma. Ophthalmology. 2014;121(5):1109-1118.
13. Wilson MW, Rodriguez-Galindo C, Billups C, Haik BG, Laningham F, Patay Z. Lack of Correlation between the Histologic and Magnetic Resonance Imaging Results of Optic Nerve Involvement in Eyes Primarily Enucleated for Retinoblastoma. Ophthalmology. 2009;116(8):1558-1563.
14. Chawla B, Sharma S, Sen S, et al. Correlation between Clinical Features, Magnetic Resonance Imaging, and Histopathologic Findings in Retinoblastoma: A Prospective Study. Ophthalmology. 2012;119(4):850-856.
15. Sirin S, Schlamann M, Metz KA, et al. High-resolution MRI using orbit surface coils for the evaluation of metastatic risk factors in 143 children with retinoblastoma. Neuroradiology. 2015;57(8):815-824.
16. Song KD, Eo H, Kim JH, Yoo S, Jeon TY. Can preoperative MR imaging predict optic nerve invasion of retinoblastoma? Eur J Radiol. 2012;81(12):4041-4045.
17. Hiasat JG, Saleh A, Al-Hussaini M, et al. The predictive value of magnetic resonance imaging of retinoblastoma for the likelihood of high-risk pathologic features. Eur J Ophthalmol. 2018:1369776408.
18. Lemke AJ, Kazi I, Mergner U, et al. Retinoblastoma - MR appearance using a surface coil in comparison with histopathological results. Eur Radiol. 2007;17(1):49-60.
19. Brisse HJ, de Graaf P, Galluzzi P, et al. Assessment of early-stage optic nerve invasion in retinoblastoma using high-resolution 1.5 Tesla MRI with surface coils: a multicentre, prospective accuracy study with histopathological correlation. Eur Radiol. 2015;25(5):1443-1452.
20. Kaliki S, Srinivasan V, Gupta A, Mishra DK, Naik MN. Clinical features predictive of high-risk retinoblastoma in 403 Asian Indian patients: a case-control study. Ophthalmology. 2015;122(6):1165-1172.
21. Shields CL, Shields JA, Baez K, Cater JR, De Potter P. Optic nerve invasion of retinoblastoma. Metastatic potential and clinical risk factors. Cancer-Am Cancer Soc. 1994;73(3):692-698.
22. Shields CL, Shields JA, Baez KA, Cater J, Potter PVD. Choroidal invasion of retinoblastoma: metastatic potential and clinical risk factors. Brit J Ophthalmol. 1993;77(9):544-548.
23. Abdel Razek AAK, ElKhamary S, Al-Mesfer S, AlKatan HM. Correlation of Apparent Diffusion Coefficient at 3T with Prognostic Parameters of Retinoblastoma. Am J Neuroradiol. 2012;33(5):944-948.
24. Finger PT, Harbour JW, Karcioglu ZA. Risk factors for metastasis in retinoblastoma. Surv Ophthalmol. 2002;47(1):1-16.
25. Rauschecker AM, Patel CV, Yeom KW, et al. High-Resolution MR Imaging of the Orbit in Patients with Retinoblastoma. Radiographics. 2012;32(5):1307-1326.
26. Razek A A, Elkhamary S. MRI of retinoblastoma. The British Journal of Radiology. 2011, 84(1005):775-84.
Figures