2952
The application of Synthetic MRI in differentiation of metastatic and reactive lymph nodes in patients with nasopharyngeal carcinoma: a preliminary study1Department of Medical Imaging, Sun Yat-sen University Cancer Center, Guangzhou, China, 2GE Healthcare, MR Research China, Beijing, China
Synopsis
Metastases of nasopharyngeal carcinoma (NPC) in lymph nodes is not uncommon at initial diagnosis, thus the differentiation of the metastatic and reactive lymph nodes is important in accurate staging and precise administration for patients. In current study, a novel MRI quantification method named synthetic MRI was applied to estimate the relaxation values of 71 and 57 metastatic and lymph nodes in 40 patients with NPC, respectively. Our results showed that the relaxation values of lymph nodes were significant different between metastatic and reactive lesions. Moreover, the ration of T1/T2 showed encouraging diagnosis efficiency in differentiation of those two lymph nodes.
Introduction
Metastases of NPC in lymph nodes are common at initial diagnosis, thus the differentiation of the metastatic and reactive lymph nodes plays an important role in accurate staging and precise administration for patients. Positron emission tomography (PET) is often used for metastatic lesions detection due to its sensitivity in detecting metabolic alteration 1, however its use is limited by the ironizing radiation and high cost. MRI may present a more preferable approach as a regular imaging approach in longitudinal treatment of NPC, but its sensitivity and specificity in distinguishing metastatic lymph nodes is unsatisfactory 2. Synthetic MRI is a novel imaging approach that offers both relaxation rate weighted imaging and quantitative relaxation weighting. It is hypothesized that the quantitative measures in synthetic MR may aid the differentiating the metastatic and reactive lymph nodes in patients with NPC, and such investigation is performed in this prospective study.Methods
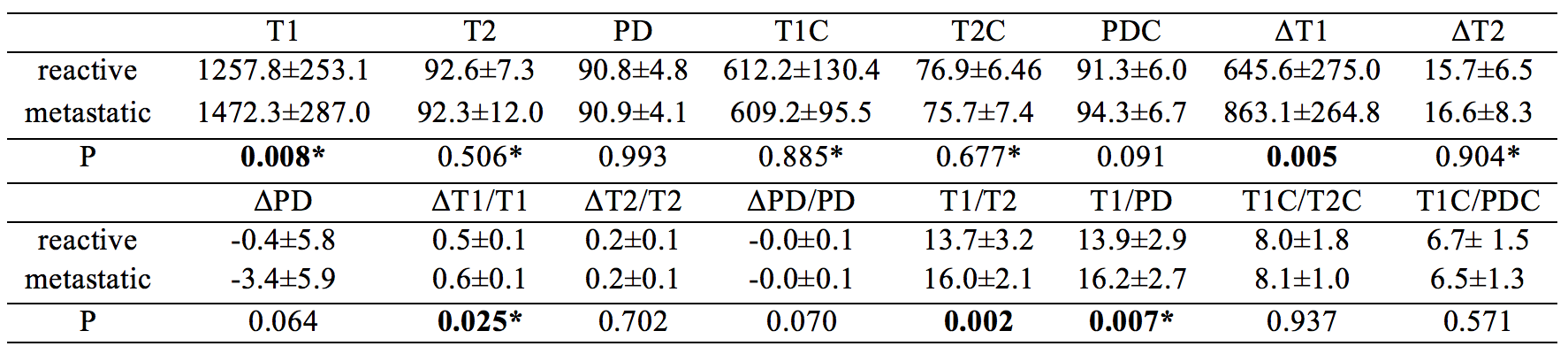
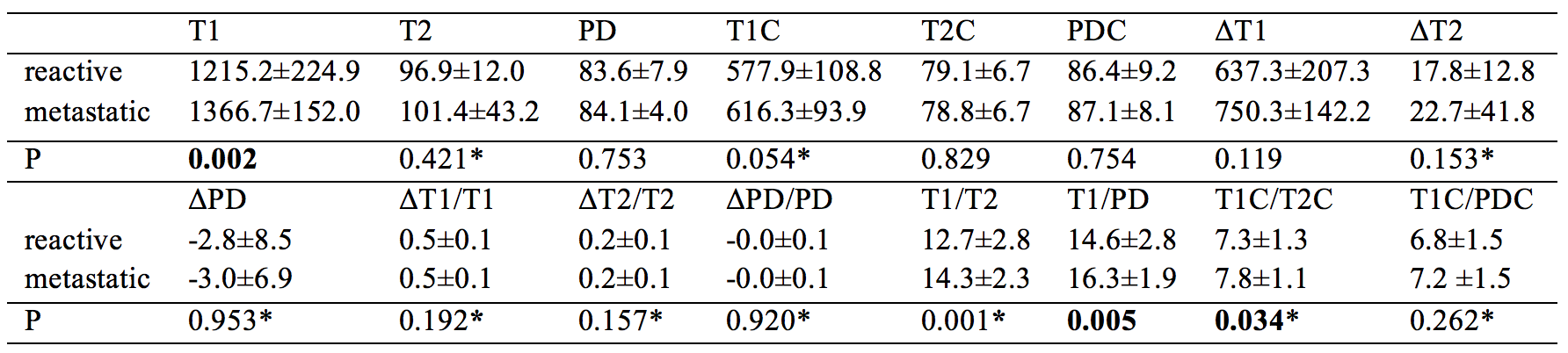
A total of 35 and 5 participants respectively with histopathology confirmed undifferentiated nonkeratinizing nasopharyngeal carcinoma and nasopharyngeal chronic inflammation were enrolled, Ethical approval and consent forms were obtained. All participants underwent MR exams on a 3.0-Tesla MR system (Signa Pioneer, GE, Milwaukee, WI, USA) consisting of routine MR sequences and synthetic MRI. Synthetic MRI were performed both prior to and after contrast injection, and the quantitative relaxation measurements of retropharyngeal (r) and cervical (c) lymph nodes including T1, T2, PD were compared. Metrics including difference values (ΔT1 = T1-T1C, ΔT2 = T2-T2C, ΔPD = PD-PDC), ratios (ΔT1/T1, ΔT2/T2, ΔPD/PD, T1/T2, T1/PD, T1C/T2C, T1C/PDC) were estimated. The metastatic lymph nodes were identified by an experienced radiologist using malignant sign in the MRI or high-metabolism in the PET/CT as references, undetermined lymph nodes were excluded. The comparison of metrics between metastatic and reactive lymph nodes were conducted using student’s t-test, or Wilcoxon Test if the values in different groups showed skewed distribution. Receiver operating characteristic (ROC) curve was used to determine the diagnosis efficiency of the metrics.Results
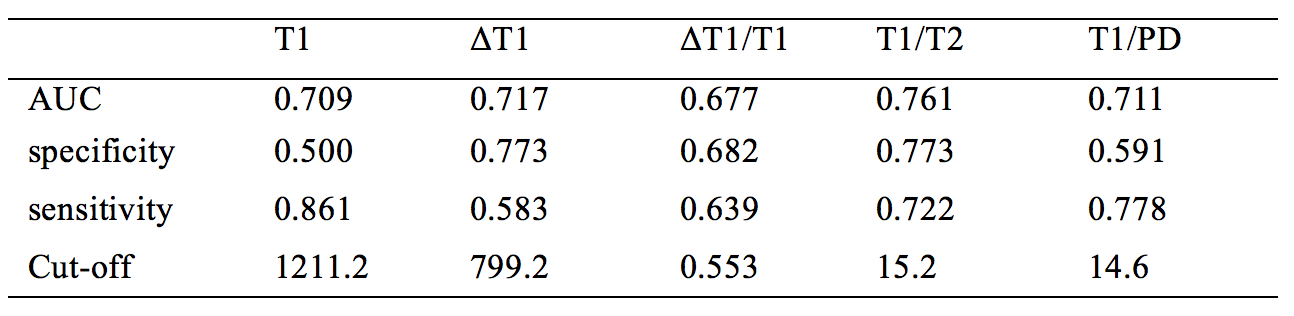
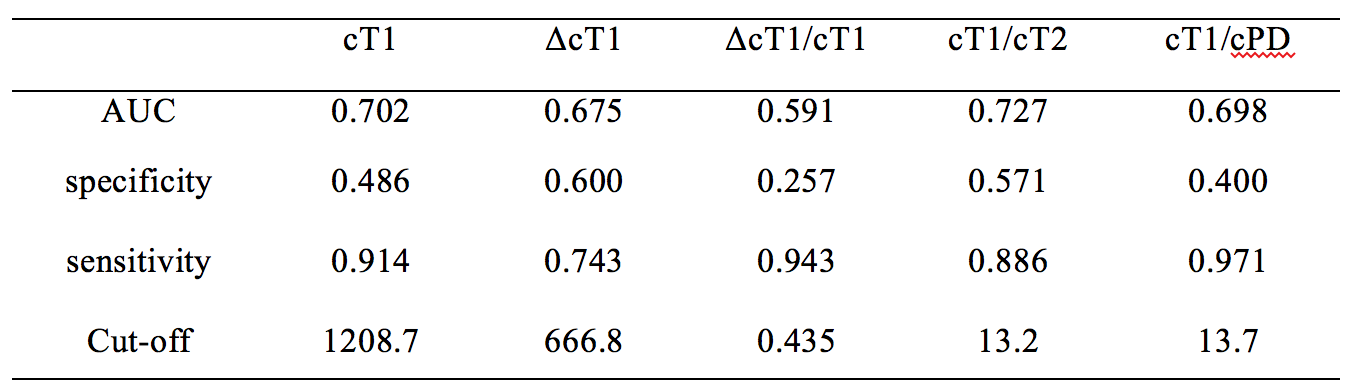
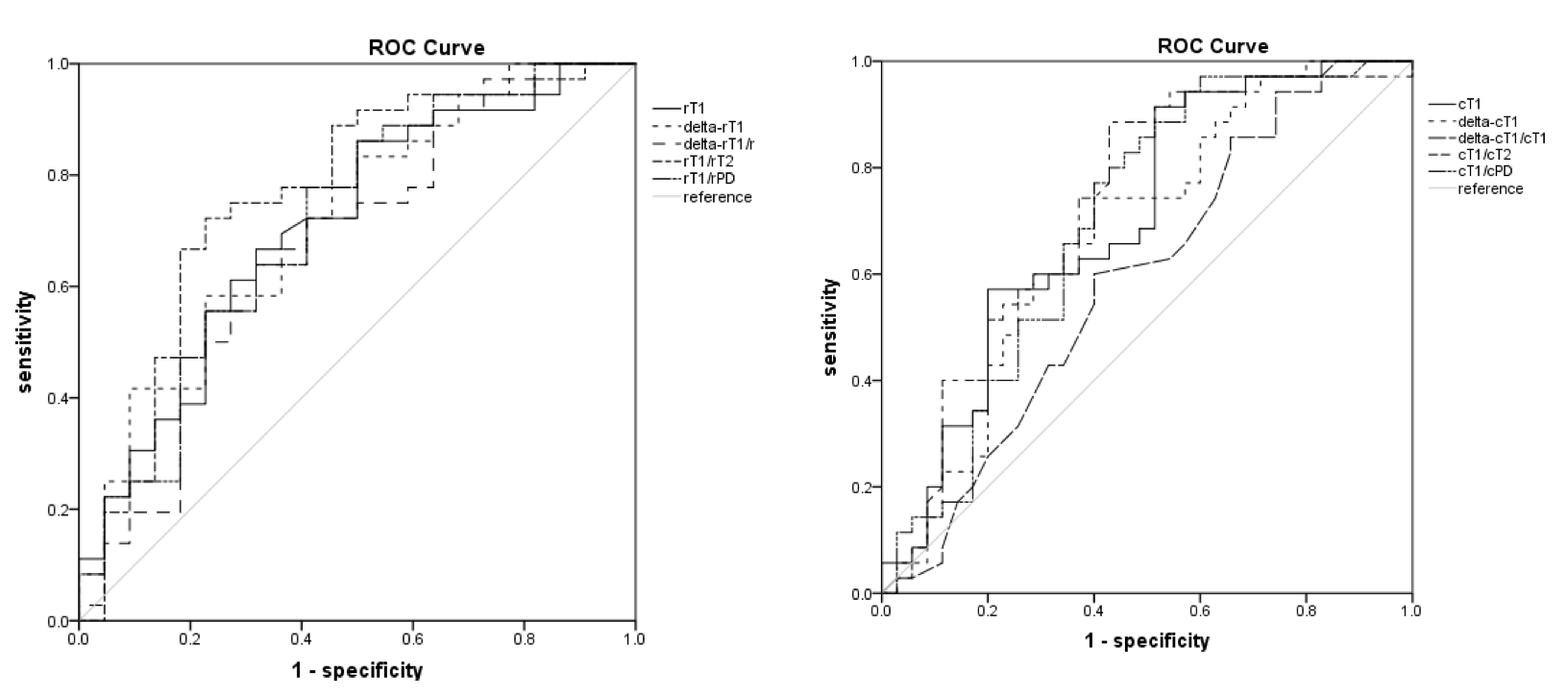
A total of 58 retropharyngeal and 70 cervical lymph nodes were evaluated, with 36 and 35 metastatic lymph nodes in each group, respectively. The T1, ΔT1, ΔT1/T1, T1/T2 and T1/PD were significantly different in the reactive and metastatic retropharyngeal lymph nodes (Table 1). Similarly, The T1, T1/T2 and T1/PD are significantly different in the reactive and metastatic cervical lymph nodes (Table 2). Furthermore, ROC curve showed the highest area under curve (AUC) at 0.761 and 0.727 with cut-off value of T1/T2 at 15.2 and 13.2 in differentiation of metastatic and reactive lymph nodes which were located at retropharynx and cervix, with the sensitivity and specificity at 0.773 and 0.727, 0.722 and 0.571, respectively (Table 3,4 and Figure 1).Discussion
It is known that the involvement of metastases may destroy the normal structure of lymph nodes, causing the alteration of size, morphology and vascularity in the lymph nodes. On the other hand, the structure and vascularity of the reactive lymphadenopathy undergo slight or no changes, which may lead to differences in the relaxation time between malignant and benign lymphadenopathy. In this work, it was observed that the following metrics showed difference: T1, ΔT1, ΔT1/T1, T1/T2 and T1/PD in retropharynx lymphadenopathy and T1, T1/T2 and T1/PD in cervical lymphadenopathy. These results indicate the longitudinal relaxation time may be more sensitive in reflecting the pathophysiological status in lesions compared to the transverse relaxation or proton density. It was also noticed that T1 of malignant lymphadenopathy was higher than that of reactive lymphadenopathy, which might be caused by the steatosis of malignant cells. In particular, the ΔT1 was also increased in malignant lesions, reflecting the abundant blood supply and vascular malformation of NPC 3, even though no statistical significance was observed in cervical lesions. Moreover, the combination of T1 and T2 (T1/T2) showed the highest diagnosis efficiency in differentiation of malignant and reactive lymphadenopathy 4.Conclusion
The quantitative relaxametry measures obtained using synthetic MRI may differentiate metastatic and reactive lymph nodes in patients with nasopharyngeal carcinoma.Acknowledgements
No acknowledgement found.References
1. Shen, G.; Zhang, W.; Jia, Z.; Li, J.; Wang, Q.; Deng, H., Meta-analysis of diagnostic value of 18F-FDG PET or PET/CT for detecting lymph node and distant metastases in patients with nasopharyngeal carcinoma. Br J Radiol 2014, 87 (1044), 20140296.
2. Sharma, M.; Bartlett, E.; Yu, E., Metastatic retropharyngeal lymph nodes in nasopharyngeal carcinoma: imaging criteria. Expert Rev Anticancer Ther 2010, 10 (11), 1703-6.
3. Ahuja, A. T.; Ying, M.; Ho, S. S.; Metreweli, C., Distribution of intranodal vessels in differentiating benign from metastatic neck nodes. Clin Radiol 2001, 56 (3), 197-201.
4. Dooms, G. C.; Hricak, H.; Moseley, M. E.; Bottles, K.; Fisher, M.; Higgins, C. B., Characterization of lymphadenopathy by magnetic resonance relaxation times: preliminary results. Radiology 1985, 155 (3), 691-7.
Figures