2951
Preliminary study on MRI arterial spin labeling and multi-b value DWI identifying the nature of retropharyngeal lymph nodes in nasopharyngeal carcinoma1Department of Diagnostic Radiology, National Cancer Center/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China, 2GE Healthcare, China, Beijing, China
Synopsis
This study using two non-invasive technique as multi-b value DWI and ASL, aimed to compare those derived parameters of metastatic RLNs from NPC patients and non-metastatic retropharyngeal lymph nodes (RLNs) from NPC patients and healthy volunteers, thus to evaluate the diagnostic value of those two series on metastatic RLNs of NPC. It was concluded that the BF, ADC and D could reflect the difference of perfusion and diffusion between metastasis and non-metastasis RLNs, especially the BF which had significant difference. Therefore, ASL and multi-b DWI would be a useful supplement method to conventional diameter criterion to determine the N stage of NPC.
Purpose
To assess the diagnostic value of parameters derived from arterial spin labeling (ASL) and multi-b value diffusion weighted imaging (DWI) on recognizing retropharyngeal lymph node (RLN) metastasis in nasopharyngeal carcinoma (NPC).Introduction
Retropharyngeal lymph node (RLN) appeared to be the first-echelon nodes in nasopharyngeal carcinoma(NPC)1, while 50.5% RLNs were metastatic for malignant involvement2. However, it is difficult to perform RNL biopsy due to its deep location in the cervical soft tissue. Therefore, the diagnosis of RLN was more dependent on imaging. At present, the criterion by imaging on diagnosis of lymph node metastasis is mainly based on the size, shape, nodal necrosis and extracapsular spread, but with a certain degree of false non-metastatic or misdiagnosis. This study using two non-invasive techniques such as multi-b value DWI and ASL, aimed to compare derived parameters of metastatic RLNs from NPC patients with those of non-metastatic RLNs from NPC patients and healthy volunteers, thus to evaluate the diagnostic value of those two series on metastatic RLNs in NPC.Material
MRI including 3D Pseudo-continuous ASL and multi-b value DWI series were performed on 52 cases of new-diagnosed NPC before treatment and 23 healthy volunteers. According to 1-3 months follow-up MRI examinations after radiotherapy, retropharyngeal lymph nodes (RLNs) were divided into metastasis as metastatic group and non-metastasis as non-metastatic group. The latter was composed of non-metastatic RLNs from patients and healthy volunteers. Measure the long and short axis, mean BF of ASL, ADC, D, D* and f of RLNs. The Independent t-test, Mann-Whitney tests and Kruskal-Wallis tests were used to carry out the comparisons among the groups, and receiver operating characteristic (ROC) curve was used to analyze the diagnostic efficiency.Results
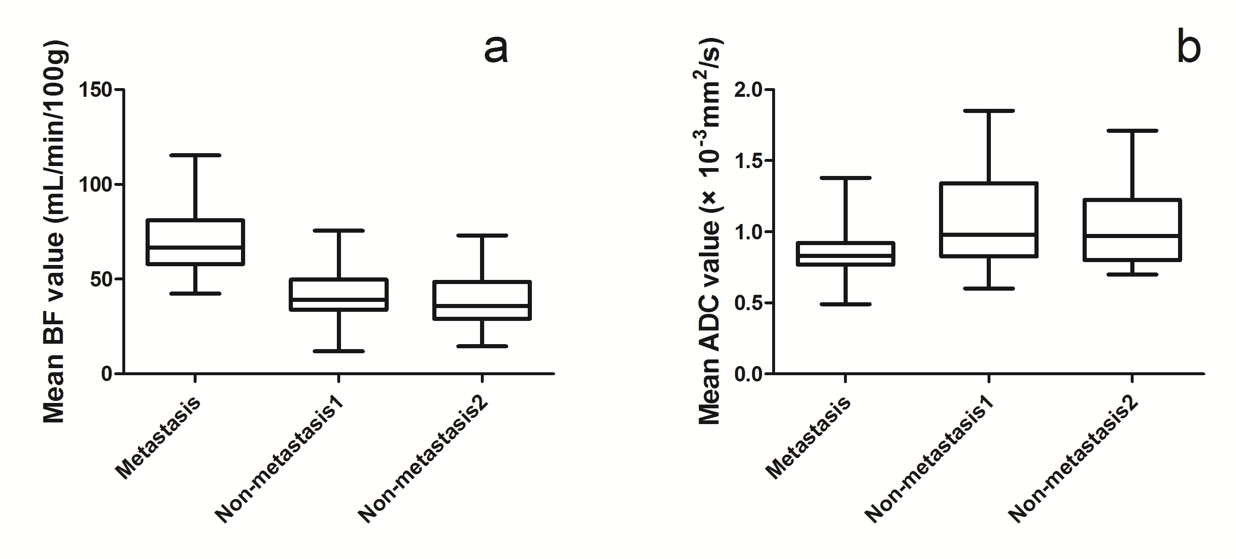
136 RLNs were divided into metastatic group (n=71) and non-metastatic group (n=65, including 33 nodes from healthy volunteers, 32 nodes from patients). The RLNs long and short axis, BF of ASL, ADC and D from multi-b value DWI demonstrated significant differences between the metastatic and non-metastatic group (P ˂0.001-0.045) with the highest AUC (0.914) on BF value. For three groups comparison, RLNs dimension, BF and ADC value were observed significant differences in metastatic groups VS. two non-metastatic groups respectively with P ˂0.001-0.004, but there was no statistically significant difference between the two non-metastatic groups (Fig.1, Fig.2). Setting the cutoff of BF larger than 49.93 mL/100g/min to distinguish metastatic RLNs from non-metastatic RLNs, the sensitivity, specificity and accuracy were 91.55%, 78.46%, and 85.29%, respectively.Discussion and Conclusion
Our results showed that metastatic RLNs had significantly higher BF and lower ADC than non-metastatic lymph nodes, indicating that metastastic RLNs had high perfusion and restricted diffusion, which were consistent with the characteristics of malignant lymph nodes and previous studies by perfusion CT on ASL3 and MRI multi-b DWI4. However, perfusion-related (f and D*) by multi-b DWI were not helpful to the diagnosis of metastatic lymph nodes, which needed further study. In conclusion, ASL and multi-b DWI would be useful supplementary methods to conventional diameter criterion in determining the N stages of NPC, especially the BF of ASL, which showed significant perfusion difference.Acknowledgements
No acknowledgement found.References
1. Wang X, Hu C, Ying H, et al. Patterns of lymph node
metastasis from nasopharyngeal carcinoma based on the 2013 updated consensus
guidelines for neck node levels. Radiother Oncol.2015, 115(1):41-45.
2. Zhang GY, Liu LZ, Wei WH, et al. Radiologic criteria of
retropharyngeal lymph node metastasis in nasopharyngeal carcinoma treated with
radiation therapy. Radiology.2010,
255(2):605-612.
3. Zhong J, Lu Z, Xu L, et al. The diagnostic value of cervical
lymph node metastasis in head and neck squamous carcinoma by using
diffusion-weighted magnetic resonance imaging and computed tomography
perfusion. Biomed Res Int.2014, 2014(2):260859.
4.Jin GQ, Yang J, Liu LD, et al. The diagnostic value of 1.5-T diffusion-weighted MR
imaging in detecting 5 to 10 mm metastatic cervical lymph nodes of
nasopharyngeal carcinoma. Medicine
(Baltimore).2016, 95(32):e4286.
Figures