2949
MRI characteristics of papillary thyroid carcinoma for the prediction of cervical lymph node metastasis1Department of Radiology, Minhang Hospital, Fudan University, Shanghai, China
Synopsis
Cervical lymph node metastasis is a known
prognostic factor in PTC. However, the greatest controversy hampering the routine application of prophylactic central neck dissection is the increased risk of
complications in thyroidectomy. In this study, we sought to investigate MRI features for predicting cervical
lymph node metastasis in papillary thyroid carcinoma. This study revealed a prediction
model built from thyroid
contour protrusion sign and poorly tumor margin in contrast enhanced imaging constituted an effective tool for
predicting PTC with cervical LNM, which was not reported in previous studies. Meanwhile, age and tumor size could be helpful to distinguish between node-negative and node-positive
papillary thyroid cancers.
Introduction
Papillary thyroid carcinoma (PTC) represents the most commonly diagnosed thyroid cancer, representing 65-88% and 87.8%-92.8% in the US and Eastern China, respectively [1, 2]. Lymph node metastasis (LNM) is found in about 30 to 80% of individuals with PTC, which enhances the odds of locoregional recurrence and might affect cancer-specific survival [3, 4]. According to ATA guidelines [5], preoperative ultrasonography (US) and fine needle aspiration biopsy (FNAB) are recommended for assessing lymph node involvement in PTC. It has been reported that US has high specificity (85%–97.4%) but low sensitivity (36.7%–61%) in detecting cervical LNM in PTC [6, 7]. Moreover, FNAB is an invasive approach and may also be limited in evaluating tumor properties exactly for invasion and metastasis [3, 8]. Magnetic resonance imaging (MRI) could provide the superior contrast of soft tissue and allows multiplane assessment. DWI has a good diagnostic value for differentiating malignant thyroid tumor from benign tumor. ADC could be used as an imaging biomarker which might guide essential initial management recommendations in PTC treatment [9]. However, the sensitivity of MRI-reported cervical LNM in PTC is still very limited (30-40%) [5]. So far, few studies have investigated MRI value for predicting cervical lymph node metastasis in PTC cases[10].Purpose
To assess MRI characteristics for predicting cervical LNM in PTC.Methods
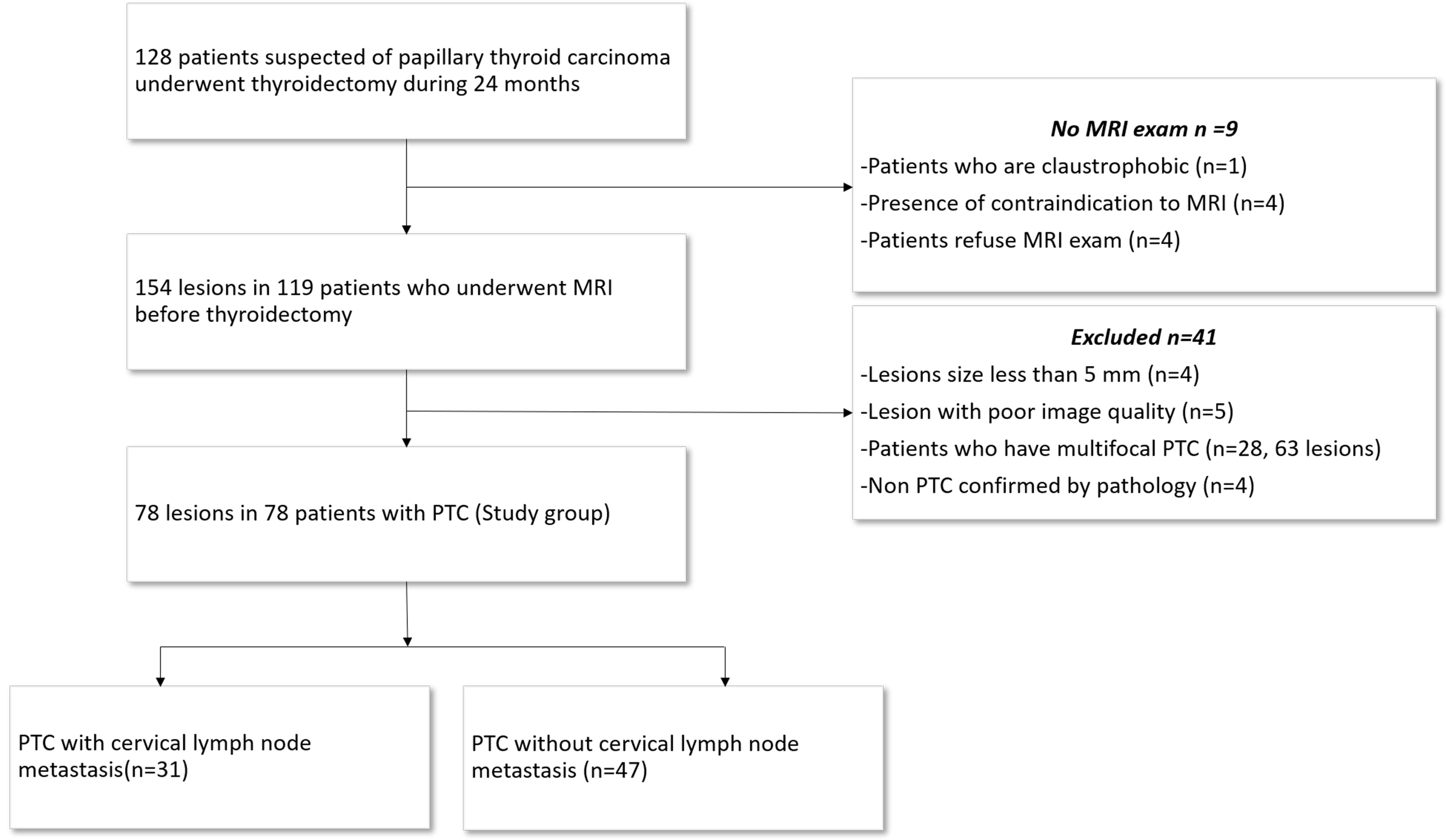
A total of 154 PTCs examined by MRI were assessed. According to inclusion and exclusion criteria, 78 tumors were included in the final analysis. Conventional MRI findings and apparent diffusion coefficient (ADC) were recorded. Descriptive statistics for LNM, sensitivity, specificity and accuracy of various parameters were obtained. Multivariate logistic regression was performed for identifying independent variables for predicting LNM. Receiver-operating characteristic (ROC) curves were used to assess the diagnostic performance of the independent variables and model.Results
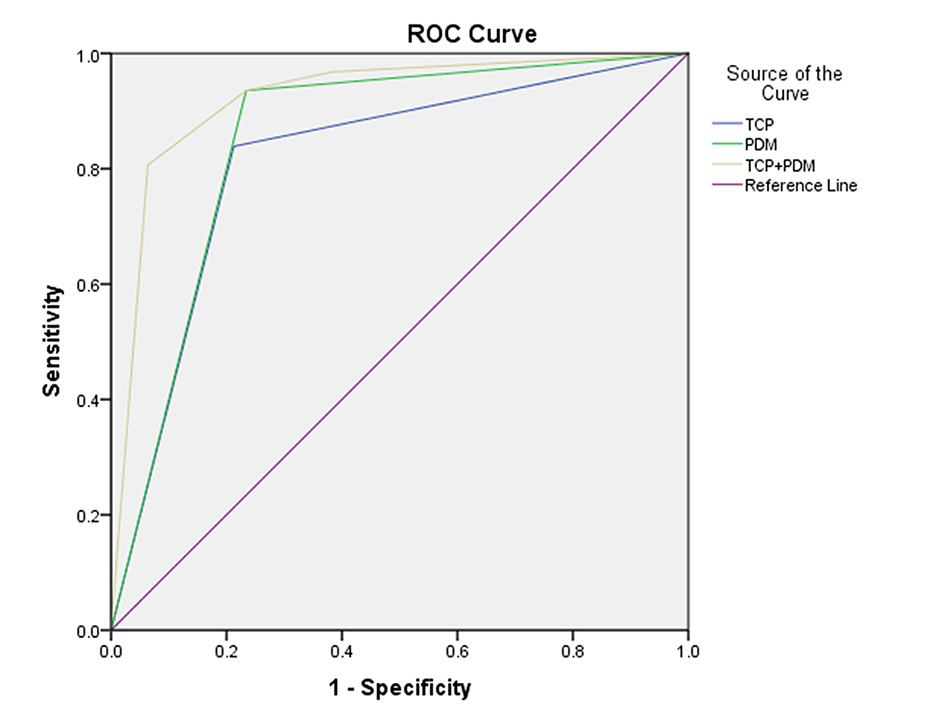
There were 31 node-positive and 47 node-negative PTCs in this study. Node-positive patients significantly differed from the node-negative group in age, tumor size, poorly defined margin in contrast-enhanced imaging and thyroid contour protrusion sign (all P<0.05). Thyroid contour protrusion sign and poorly defined tumor margin were identified as independent predictive factors of LNM in PTC (Both P<0.05), with area under the curves (AUCs) of 0.81 and 0.85, accuracies of 0.81 and 0.83. When the independent factors were combined, the diagnostic performance was improved with an AUC of 0.86 and an accuracy of 0.87.Discussion
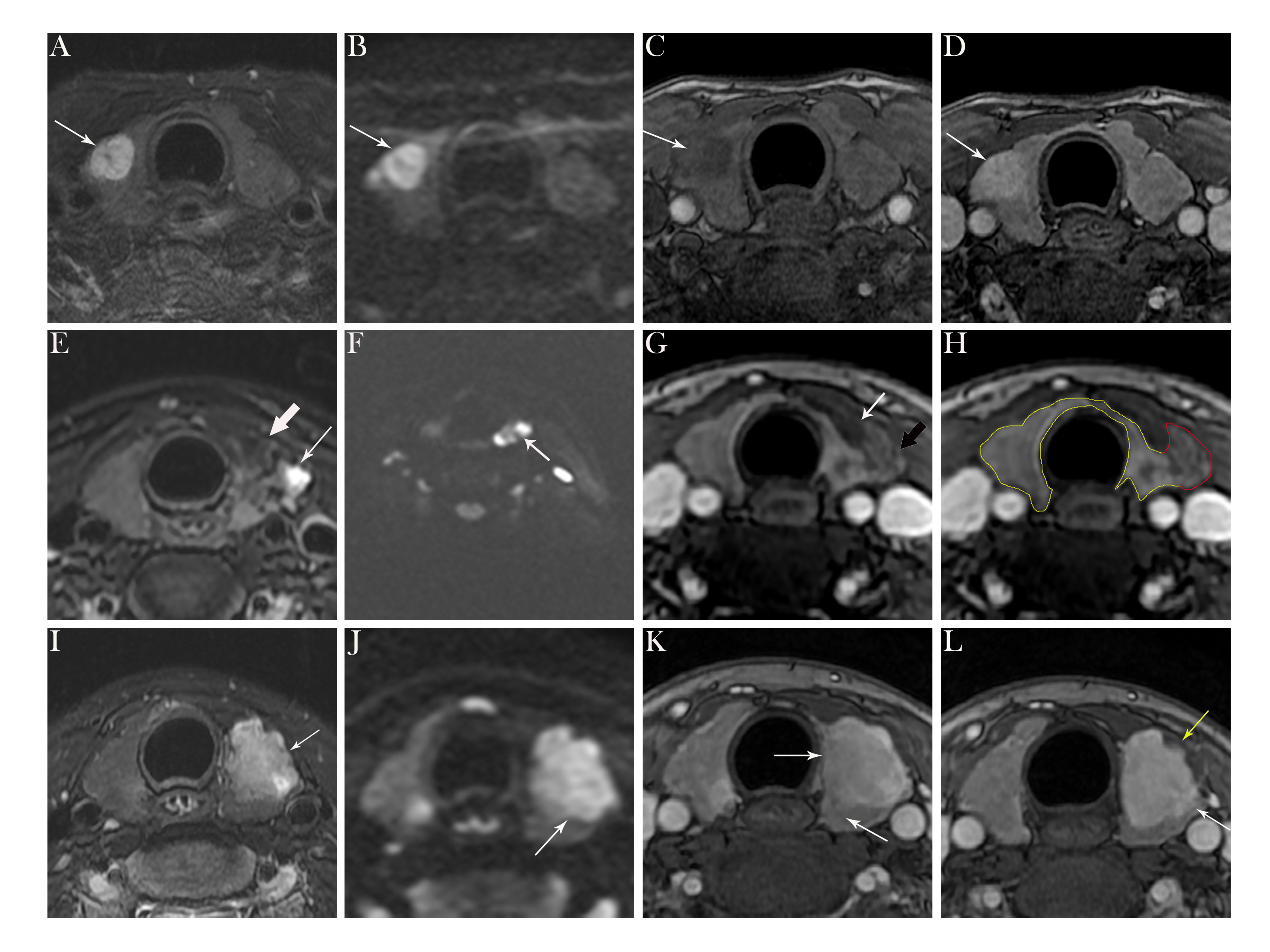
Cervical LNM is a known prognostic factor in PTC[11]. However, the greatest controversy hampering the application of prophylactic central neck dissection is the increased risk of complications in thyroidectomy [12]. This study revealed a prediction model built from thyroid contour protrusion sign and poorly tumor margin constituted an effective tool for predicting PTC with cervical LNM, which was not reported in previous studies. A previous study [10] demonstrated MRI provides useful data regarding tumor biology in thyroid cancer. Some investigators [9, 13] have determined MRI properties segregating lowly from highly aggressive PTC lesions. The current work demonstrated the significance of tumor margin in the prediction of cervical lymph node metastasis. Commonly, poorly defined tumor margins in contrast-enhanced imaging imply tumor cells could infiltrate into the surrounding non-cancerous thyroid parenchyma, with incomplete peripheral fibrous stroma, reflecting PTC invasiveness. Histologically, a blurred border separates the cancer and surrounding noncancerous thyroid tissue. Otherwise, a well-defined margin could be correlated with low aggressiveness of PTC. In this study, thyroid contour protrusion sign was another important independent indicator for the prediction of node-positive PTCs, with an accuracy of 81.3%. According to the 2015 version of the ATA guideline [5], high risk patients usually have gross extrathyroidal extension (ETE), as defined previously [9]. ETE is correlated with the risk of differentiated thyroid carcinoma recurrence. In the present study, thyroid contour protrusion sign was a morphological term, histopathologically like ETE. We speculated that nodal-positive PTCs showing a high aggressive behavior could grow heterogeneously local growth is faster, e.g. in the thyroid capsule, reflecting imaging data. PTC with cervical lymph node metastasis could be correlated with that with ETE, which all showed highly aggressive histopathological behavior. When the two features mentioned above co-occurred, MRI had a very high specificity (93.6%) in predicting lymph node metastasis in PTC, with an accuracy of 87.2%. The two features were indeed subjective dependent upon the radiologist's experience. Despite this, a satisfactory interobserver agreement was obtained between both examiners (Cohen k of 0.871 and 0.872) in this study.Conclusion
Thyroid contour protrusion sign and poorly defined tumor margin in contrast-enhanced imaging could be two important predicted findings for cervical LNM in PTC.Acknowledgements
We thank all members of the Department of Radiology, Minhang Branch, Zhongshan Hospital, Fudan University(Bin Song, Ran Wei, Wenjuan Hu, Lanyun Wang, Yi Ding, Zedong Dai, Xilin Sun)and all members of the Department of Pathology and General Surgery for helpful discussions and invaluable help in manuscript preparation.References
1. Xiang J, Wu Y, Li DS, Shen Q, Wang ZY, Sun TQ, et al. New clinical features of thyroid cancer in eastern China. J Visc Surg 2010,147:e53-56.
2. Enewold L, Zhu K, Ron E, Marrogi AJ, Stojadinovic A, Peoples GE, et al. Rising thyroid cancer incidence in the United States by demographic and tumor characteristics, 1980-2005. Cancer Epidemiol Biomarkers Prev 2009,18:784-791.
3. Jianyong L, Zhihui L, Rixiang G, Jingqiang Z. Using a nomogram based on preoperative serum fibrinogen levels to predict recurrence of papillary thyroid carcinoma. BMC Cancer 2018,18:390.
4. Mehanna H, Al-Maqbili T, Carter B, Martin E, Campain N, Watkinson J, et al. Differences in the recurrence and mortality outcomes rates of incidental and nonincidental papillary thyroid microcarcinoma: a systematic review and meta-analysis of 21 329 person-years of follow-up. J Clin Endocrinol Metab 2014,99:2834-2843.
5. Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016,26:1-133.
6. Liu X, Ouyang D, Li H, Zhang R, Lv Y, Yang A, et al. Papillary thyroid cancer: dual-energy spectral CT quantitative parameters for preoperative diagnosis of metastasis to the cervical lymph nodes. Radiology 2015,275:167-176.
7. Kim E, Park JS, Son KR, Kim JH, Jeon SJ, Na DG. Preoperative diagnosis of cervical metastatic lymph nodes in papillary thyroid carcinoma: comparison of ultrasound, computed tomography, and combined ultrasound with computed tomography. Thyroid 2008,18:411-418.
8. Liu Y, Zhou H, Yang P, Zhou Y, Wu J, Chen C, et al. Contrast-enhanced ultrasonography features of papillary thyroid carcinoma for predicting cervical lymph node metastasis. Exp Ther Med 2017,14:4321-4327.
9. Lu Y, Moreira AL, Hatzoglou V, Stambuk HE, Gonen M, Mazaheri Y, et al. Using diffusion-weighted MRI to predict aggressive histological features in papillary thyroid carcinoma: a novel tool for pre-operative risk stratification in thyroid cancer. Thyroid 2015,25:672-680.
10. Schob S, Meyer HJ, Dieckow J, Pervinder B, Pazaitis N, Hohn AK, et al. Histogram Analysis of Diffusion Weighted Imaging at 3T is Useful for Prediction of Lymphatic Metastatic Spread, Proliferative Activity, and Cellularity in Thyroid Cancer. Int J Mol Sci 2017,18.
11. Sun R, Zhang H, Liu K, Fan J, Li G, Song X, et al. Clinicopathologic Predictive Factors of Cervical Lymph Node Metastasis in Differentiated Thyroid Cancer. Acta Otorrinolaringol Esp 2018,69:149-155.
12. Carling T, Carty SE, Ciarleglio MM, Cooper DS, Doherty GM, Kim LT, et al. American Thyroid Association design and feasibility of a prospective randomized controlled trial of prophylactic central lymph node dissection for papillary thyroid carcinoma. Thyroid 2012,22:237-244.
13. Song B, Wang H, Chen Y, Liu W, Wei R, Dai Z, et al. Magnetic resonance imaging in the prediction of aggressive histological features in papillary thyroid carcinoma. Medicine (Baltimore) 2018,97:e11279.
Figures