2946
Incidence of enlarged perivascular spaces six-months after aneurysmal subarachnoid hemorrhage: a retrospective MR study1Radiology, Santa Maria del Carmine Hospital, Rovereto, Italy, 2Center for Mind/Sciences, CIMeC, Rovereto, Italy, 3Neurosurgery, University of Southampton, Southampton, United Kingdom, 4Clinical neurosciences, University of Southampton, Southampton, United Kingdom, 5Neuropathology, Faculty of medicine, Southampton, United Kingdom, 6Neurosurgery, University Hospital Southampton, Southampton, United Kingdom
Synopsis
One of the major complications of subarachnoid hemorrhage (SAH) is vasospasm which could last days. This could affect the clearance of interstitial fluid (ISF) from the brain parenchyma by restricting its movement along the intramural periarterial drainage (IPAD) pathway. This would result in dilated perivascular spaces (PVS) which have been shown to be an MR biomarker of failure of IPAD. We explore the hypothesis that patients with hemorrhage will present with an increased prevalence of PVS at six months.
BACKGROUND
Annual incidence of aneurysmal subarachnoid hemorrhage (aSAH) is 9.1/100,000 population. Microvascular spasm can lead to one of the major complication of aSAH known as delayed ischemic neurological deficit, affecting 20-30% of patients. This could affect the clearance of interstitial fluid (ISF) from the parenchyma. ISF and solutes are eliminated from the parenchyma along the walls of the capillaries and arteries via the intramural periarterial drainage pathway (IPAD) 1. The motive force for IPAD appears to be derived from the strength of arterial smooth muscle cell contraction. Dilated PVS are a sign of failure of fluid drainage through IPAD2. There is also evidence that there is an increased risk of dementia amongst survivors of SAH3,4. In this study we explore the hypothesis that after SAH there is increased prevalence of dilated PVS by reviewing magnetic resonance scans of patients with SAH and without SAH.MATERIALS AND METHODS
We retrospectively collected MRI data from 38 patients with aSAH (Fisher 3 and 4) performed at six months (Group A) and from 17 patients with asymptomatic aneurysms and no prior history of brain hemorrhage (Group B). MR was performed on a Siemens 3T scanner and data was evaluated using the following sequences: T2-weighed SPACE (TR/TE 3200/210ms; 1mm slice thickness; no gap) and T1-MPRAGE (TR/TE 2200/2.45ms; 1mm slice thickness; no gap). All data was anonymized and examined by an external experienced neuroradiologist. All scans were rated for the prevalence of prominent PVS and their location. The presence of lacunes, gliotic foci were also noted to identify small vessel disease and was ranked according to Fazekas classification.RESULTS
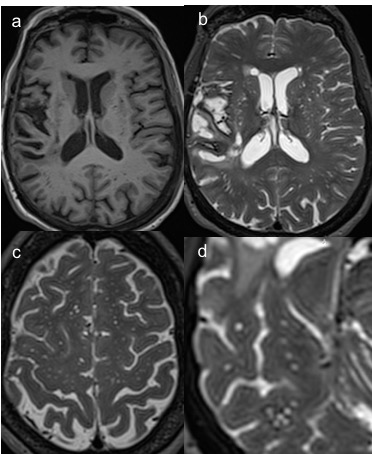
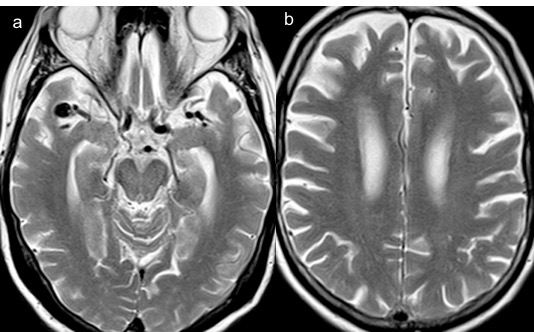
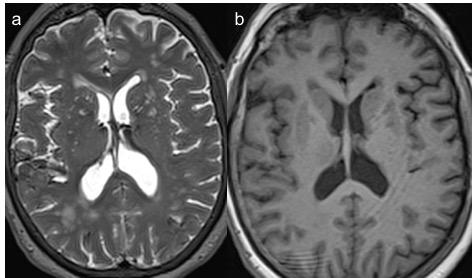
The two groups were matched for age and sex. There was a significant difference (p=0.0002) in the prevalence of prominent PVS in patients in Group A and B (76.3% vs 23.5% respectively). The distribution of PVS was mostly seen in either the basal ganglia only or both basal ganglia and centrum semiovale (CSO) (52.6% and 26.3%). The presence of PVS in basal ganglia alone was also significantly increased (p=0.004) in patients who suffered SAH with respect to patients in Group B. The presence of white matter hyperintensities (WMH) or lacunes was not significantly different among the two groups. MR representative images for a patient in Group A and Group B are illustrated in Figures 1, 2 and 3.DISCUSSION
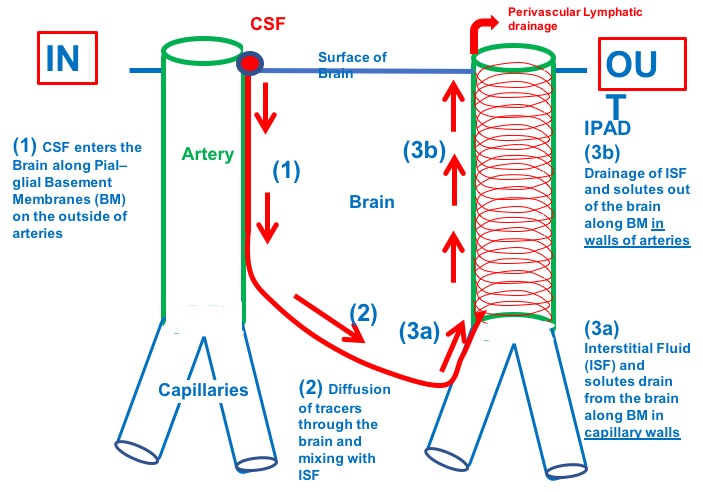
In this study the prevalence of dilated PVS was significantly higher in patients with SAH as compared to controls. This suggests that there is impaired drainage of ISF. A possible mechanism is that fibrin or blood breakdown products from CSF can enter the glymphatic pathway consisting of pial basement membrane thereby interfering with arterial constriction and IPAD (Figure 4). Future studies should aim to test this in experimental models. Therapeutic strategies should consider prevention of dementia due to failed drainage.Acknowledgements
We are grateful to Prof. Roy Weller for his precious suggestions.References
1. Carare RO, Bernardes-Silva M, Newman TA, Page AM, Nicoll JAR, Perry VH, et al. Solutes, but not cells, drain from the brain parenchyma along basement membranes of capillaries and arteries: significance for cerebral amyloid angiopathy and neuroimmunology. Neuropathol Appl Neurobiol. 38 ed. Blackwell Publishing Ltd; 2008 Apr;34(2):131–44.
2. Weller RO, Hawkes CA, Kalaria RN, Werring DJ, Carare RO. White Matter Changes in Dementia: Role of Impaired Drainage of Interstitial Fluid. 2014 Dec 17;25(1):63–78.
3. Corraini P, Henderson VW, Ording AG, Pedersen L, Horváth-Puhó E, Sørensen HT. Long-Term Risk of Dementia Among Survivors of Ischemic or Hemorrhagic Stroke. Stroke. 2017 Jan;48(1):180–6.
4. Banerjee G, Kim HJ, Fox Z, Jäger HR, Wilson
D, Charidimou A, et al. MRI-visible perivascular space location is associated
with Alzheimer's disease independently of amyloid burden. Brain. 2017 Feb
17;140(4):1107–16.
Figures