2945
Evaluating of intracranial artery dissection using 3D-SNAP high resolution magnetic resonance:the prospective study1Shaanxi Provincial People`s Hospital, xi`an, China, 2Clinical science, Philips Healthcare China, Beijin, China
Synopsis
The characteristics of intracranial artery dissection were firstly observed using three dimensional simultaneous non-contrast angiography and intra plaque hemorrhage (3D-SNAP) high-resolution magnetic resonance imaging, including intramural hematoma, double lumen and intimal flap. 43 patients were enrolled. The discovery rate of intramural hematoma, false lumen thrombosis were significantly higher in the intracranial artery dissection by 3D-SNAP than other MRI sequences. The discovery rate of double lumen and intimal flap using 3D-SNAP were minor superior to CE-T1WI sequences. The diagnosis efficiency of 3D-SNAP sequences was only lower CE-T1WI, it was the highest diagnostic efficacy in combination with 3D-SNAP and CE-T1WI sequences. Therefore, the application of 3D-SNAP would rise diagnosis rate of intracranial artery dissection, and it may become the first-line screening technology to evaluate the risk factors of stroke caused for intracranial artery dissection.
Introduction
Intracranial arterial dissection (ICAD) is a major cause for stroke in young and middle-aged people, and often causes serious complications with ischemia and hemorrhage. At present, the intraluminal imaging (DSA, CTA and MRA) cannot fully reveal the direct signs of intracranial artery dissection, their can diagnose 32%-50% in ICAD, susceptibility weighted imaging (SWI) cannot clearly observe intramural hematoma, false lumen thrombosis and duble lumen caused for magnetic sensitive artifact, slow blood flow, the all factors will reduces to the discovery rate of intracranial artery dissection [1]. However, The SNAP sequence can simultaneouly provide a full 3D luminal MRA and a naturally registered 3D intraplaque hemorrhage (IPH) visualization in a single acquisition. It can obtain good contrast among lumen, wall and IPH in plaque due to suppress blood flow signal [2]. The histopathology of intracranial arterial dissection is intramural hematoma, double lumen and intimal flap due to the intimal tear and vasa vasorum of the outer and middle membranes rupture. Therefore, the purpose of this study is to explore the pathological features of intracranial artery dissection using 3D-SNAP, to improve the diagnostic accuracy and guide clinic treatment.Methods
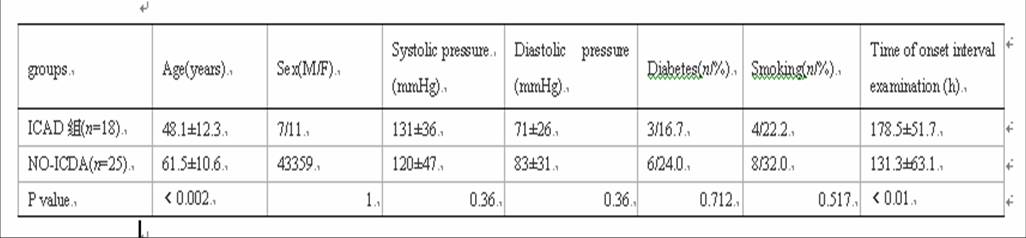
We prospectively recruited patients with transient ischemic attack(TIA) or acute neurological deficit compatible with headache and dizziness from Jan 2015 to Mar 2018, patients with a history of trauma, poor image quality and clinical findings suggestive of vasculitis were excluded from study. The study was approved by local IRB. They were devided into the ICAD group (n=18) and the non-dissection group (n=25). The inclusion criteria of ICAD were as follows [3]: (a) evidence of VAD on digital subtraction angiography (DSA), (b) findings of double-lumen sign, intimal flap or intramural hematoma. The inclusion criteria of nondissection group were as follows: (a) ischemic stroke, (b) no evidence of pathognomonic ICAD imaging. All patients were performed TOF-MRA, T1WI-VISTA, T2WI, 3D-SNAP and CE-T1WI using Philips Ingenia 3.0 T MRI (ingenia, Philips Medical Systems, The Netherlands),following parameters: TR/TE:10/5ms, FOV=160*160mm2, acquisition matrix=512X512, image resolution=1*1*1mm2, acceleration factor=2, slice thickness= 0.5 mm (no gap), acquisition time approximately 3.32 minutes. Image analysis: The 3D-SNAP original data were imported into PHILIPS MR WorkSpace postprocessing workstation to generate axial view, coronal view, surface reconstruction and minimum density projection. The all patients were double-blinded analyzed image findings every sequences. The Kappa analysis was used to evaluate the consistency of the 2 physicians. The independent sample t test or chi-square test was used for clinic data, image findings between ICAD group and the non-dissection group. ROC curve was used to evaluate diagnostic efficiency of each sequence in intracranial artery dissection. P<0.05 is considered statistically significant.Results
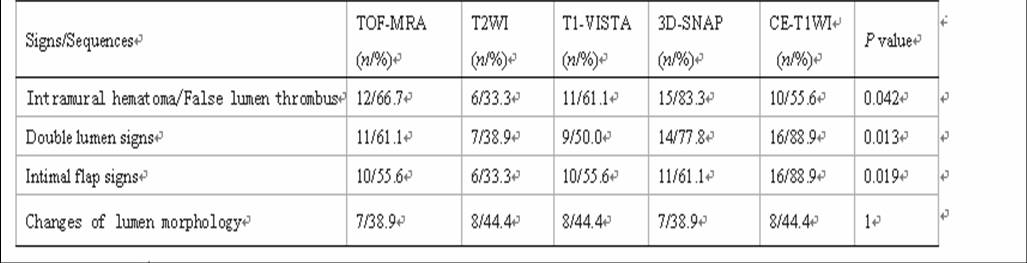
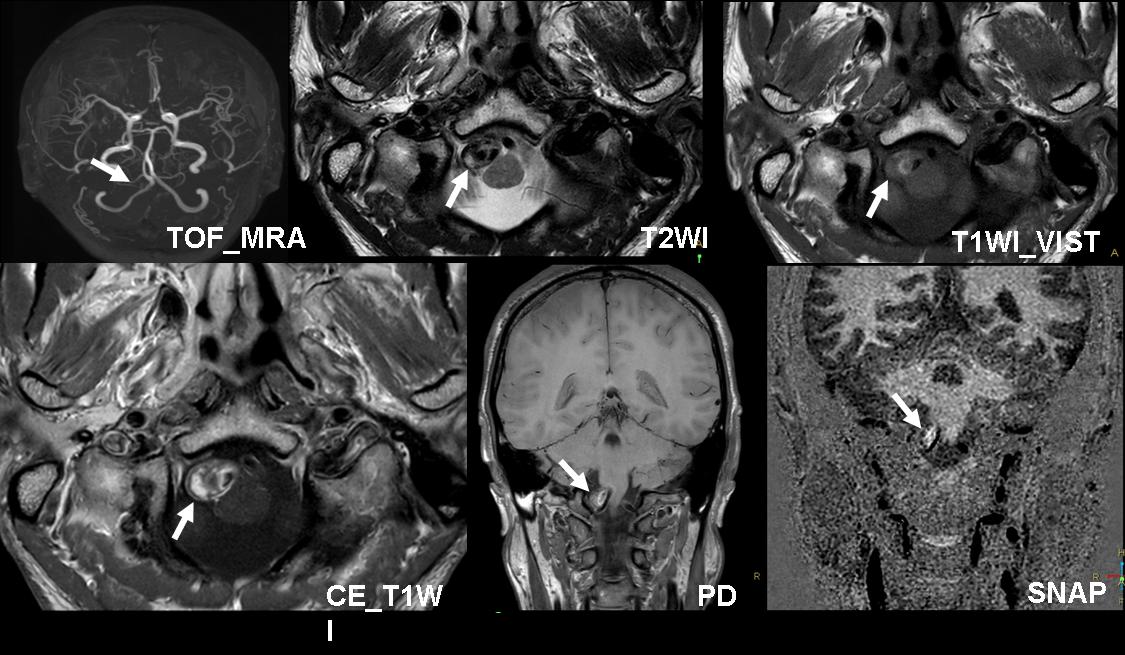
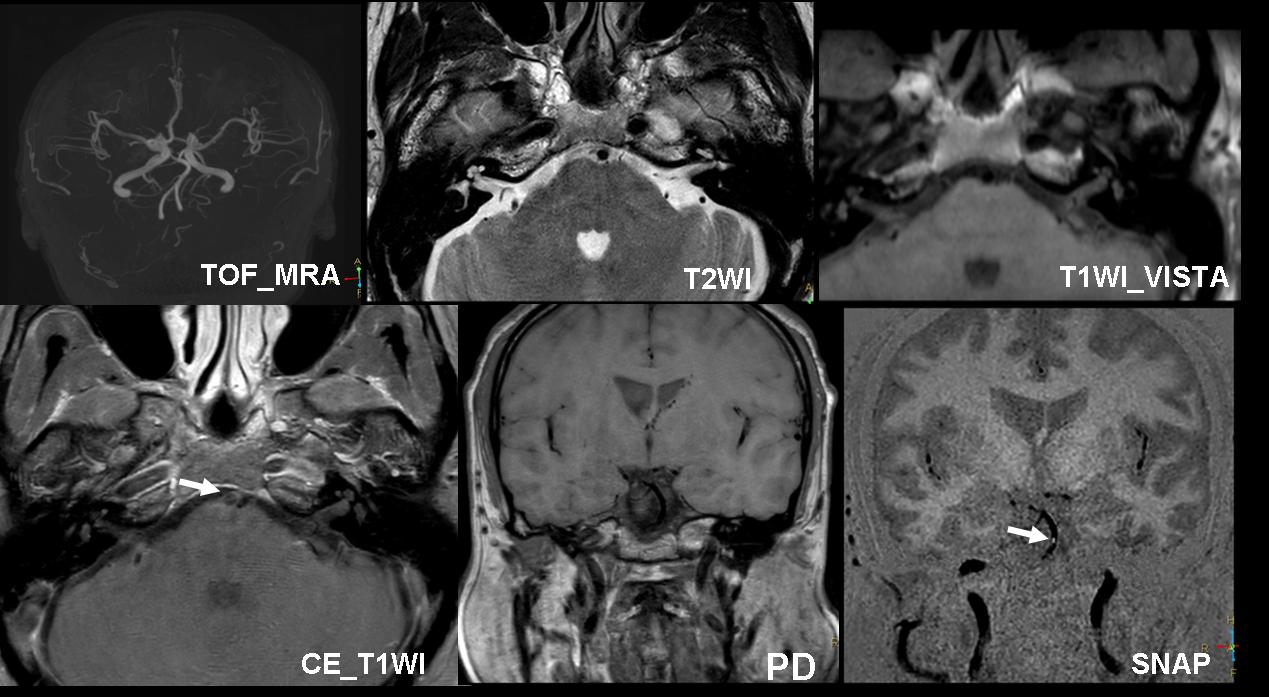
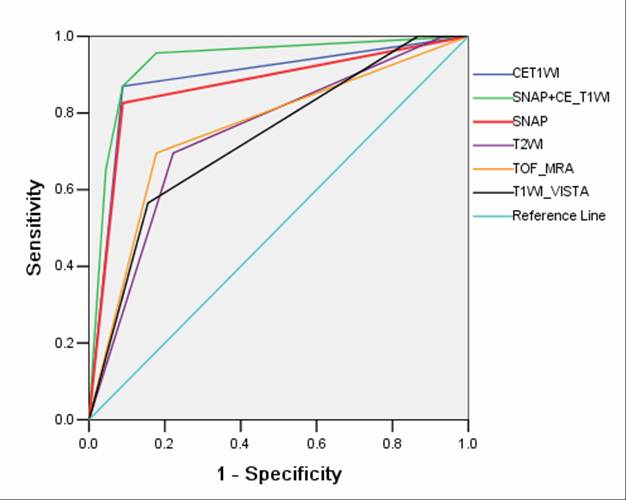
The age between ICAD group and the non-dissection was statistically significant (P<0.05) (Tab.1).There was significant difference in the displaying rates of intramural hematoma, double lumen, intimal flap signs in ICAD on TOF-MRA, T2WI, T1WI-VISTA, SNAP and CE-T1WI(Tab.2,Fig.1). The SNAP was the most sensitive method for diagnosis of intramural hematoma, the CE-T1WI was the most sensitive to display double lumen and intimal flap signs(Fig.2). Areas of TOF-MRA, T2WI, T1WI-VISTA, SNAP, CE-T1WI, SNAP combined with CE-T1WI under ROC curves to diagnose ICAD were 0.663, 0.492, 0.729, 0.741, 0.752 and 0.824, respectively (Fig.3).Discussion
Conclusion
Acknowledgements
The authors would like to thank Philips Healthcare for their technical assistance.References
[1]. Han M, Rim N J, Lee J S, et al. Feasibility of high-resolution MR imaging for the diagnosis of intracranial vertebrobasilar artery dissection[J]. European Radiology, 2014, 24(12):3017-3024.
[2].Wang J, Börnert P, Zhao H, Hippe DS, Zhao X, Balu N, et al. Simultaneous noncontrast angiography and intraplaque hemorrhage (SNAP) imaging for carotid atherosclerotic disease evaluation. Magn Reson Med. 2013; 69(2):337–345
[3].Maruyama H, Nagoya H, Kato Y, et al. Spontaneous cervicocephalic arterial dissection with headache and neck pain as the only symptom. J Headache Pain 2012;13:247-53.
Figures