2942
Assessment of obstructive sleep apnea on cerebrovascular health in children with obesity using MRI1University of Toronto, Toronto, ON, Canada, 2Translational Medicine, The Hospital for Sick Children, Toronto, ON, Canada, 3Medical Imaging, University of Toronto, Toronto, ON, Canada
Synopsis
Obstructive sleep apnea (OSA) is a significant contributor to co-morbid disease in obese children. Cerebral endothelial dysfunction and neurocognitive deficits have been linked to obesity-related OSA. However, the effect of the chronic hypoxic environment caused by untreated OSA on cerebrovascular health in the pediatric population remains unclear. Cerebrovascular reactivity (CVR) measured with BOLD MRI in response to a CO2 stimulus is a useful tool in the clinical assessment of cerebrovascular disease. This study seeks to understand the effect of OSA on the cerebrovascular health in obese pediatric patients through MRI assessment.
Introduction
With extremely prevalent rates of obesity currently affecting today’s children, the incidence of obesity-related obstructive sleep apnea (OSA) is also increasing1. OSA is characterized by intermittent episodes of nocturnal hypoxia, hypercapnia and sleep disruption and is, therefore, a significant contributor to co-morbid disease in obese children. These features of OSA lead to oxidative damage of endothelial cells, increase cerebral blood flow (CBF) and therefore disrupts the vasodilatory capacity and increases the risk of cerebrovascular dysfunction2. The obese OSA population also experience impaired neurocognitive ability and poor school performance which can be associated with cerebrovascular damage3. Non-invasive magnetic resonance imaging strategies can assess vessel distensibility, and therefore vasodilatory capacity, by quantifying the relative changes in CBF in response to a vasoactive stimulus4. The resulting measure, cerebrovascular reactivity (CVR), can help us understand the mechanism of cerebrovascular injury and can serve a useful tool in the clinical assessment of cerebrovascular health. We hypothesize that CVR measures will decrease with higher CBF and with increasing severity of OSA, determined by the Obstructive Apnea-Hypopnea Index (OAHI), in obese children.Methods
33 obese patients between 9 and 18 years old were included and received overnight polysomnography tests to assess severity of OSA. They were classified as having no OSA (n=10, OAHI<1.5), mild-OSA (n=9, 1.5≤OAHI≤5.0) or moderate-to-severe OSA (n=14, OAHI>5.0). Each patient was then imaged on a 3T MRI scanner using a 32-channel head coil. CVR data were acquired using a blood-oxygen level dependent (BOLD) sequence during a computer-controlled administration of a vasoactive stimulus through a rebreathing mask. The BOLD CVR images were acquired with TR/TE = 2000/40ms, FOV = 220mm, matrix size = 64×64, slices = 25, slice thickness = 4.5mm, volumes = 240, time = 8 minutes. The stimulus paradigm alternated between 60 seconds of normocapnia (PETCO2 = 40mmHg, PETO2 = 100mmHg) and 45 seconds of hypercapnia (PETCO2 = 45mmHg, PETO2 = 100mmHg). CBF was measured using a PICORE arterial spin labeling sequence and quantified with the vendor pipeline. Additionally, a high resolution MPRAGE anatomical scan was performed for tissue classification. The BOLD CVR and CO2 data were transferred to an independent workstation for post-processing and analysis. High resolution CVR maps were computed using FSL v1.4 as previously described5. CVR maps for each subject were co-registered to the corresponding anatomical scan and then average across grey and white matter regions. SPSS v23 was used to perform comparisons between OSA groups and Pearson correlation analysis on the resulting data.Results
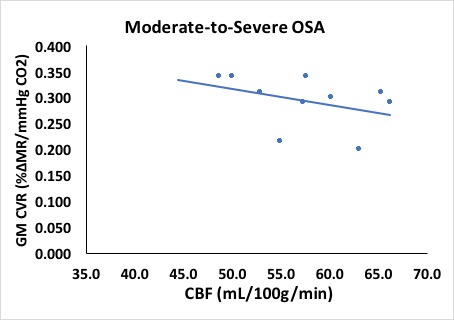
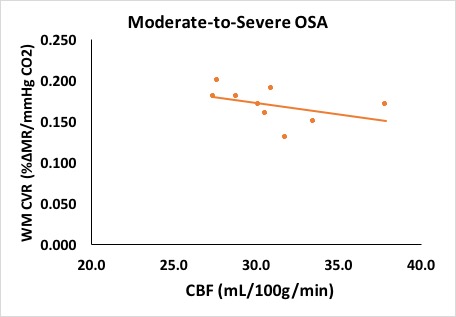
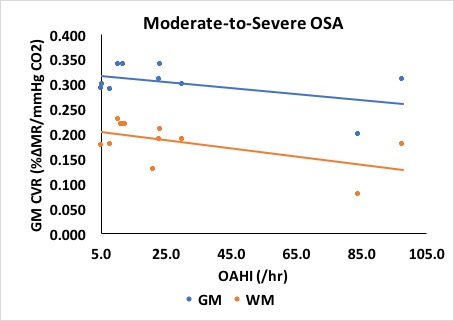
Patients in the moderate-to-severe OSA group had higher GM CBF measures compared to the no OSA and mild OSA groups (56.1, 50.4 and 50.9 mL/100g/min respectively, p<0.05). CVR measures were similar across the no, mild and moderate-to-severe groups (0.301, 0.273 and 0.285 %ΔMR/mmHg CO2, respectively). Higher CBF was inversely associated with CVR in obese patients with moderate-to-severe OSA for both GM [Figure 1] and WM [Figure 2] (r=-0.331 and r=-0.590, respectively). Furthermore, in patients with moderate-to-severe OSA, a decline in CVR was observed for both GM and WM [Figure 3] when plotted against the Obstructive Sleep Apnea Index (OAHI) (r=-0.297 and r=-0.508, respectively).Discussion
In this study, we have demonstrated higher CBF values in obese patients with moderate-to-severe OSA compared to those with no or mild OSA. Reduced CVR in children with obesity and moderate-to-severe OSA may be exposed to a higher risk of cerebrovascular damage. If left untreated, this may present behaviourally as neurocognitive deficits and serious vasculopathies such as stroke. Further studies are needed to confirm our results in a larger cohort and to assess the effectiveness of CPAP therapy.Acknowledgements
No acknowledgement found.References
1) Roberts, K.C., et al., Overweight and obesity in children and adolescents: Results from the 2009 to 2011 Candian Health Measures Survey. Health Reports.
2) Cereda CW et al.: Stroke 2013; 44:1175–8.
3) Torelli F et al.: Neuroimage 2011; 54:787–93.
4) Yonas H, Pindzola RR: Cerebrovasc Brain Metab Rev 1994; 6:325–40.
5) Leung J, Kosinski PD, Croal PL, et al. J Physiol 2016;594(10):2681-9.
Figures