2941
Plaque Characteristics Contribute to Misery Perfusion in Patients with Symptomatic Middle Cerebral Artery Stenosis: A Study of Combined Perfusion MR and High-Resolution Vessel Wall Imaging1Radiology Department, First Clinical College,Tianjin Medical University, Tianjin, China, 2Radiology Department, Tianjin First Central Hospital, Tianjin, China
Synopsis
High-resolution vessel wall imaging(HR-VWI) is an novel technique used to assess intracranial artery stenosis, and it has been useful in clinical practice. In addition, time-to-maximum (Tmax) maps, derived from PWI, are increasingly being used in studies of ischemic stroke, and can provide more prominent cerebral hemodynamic information. Our study aimed to investigate the plaque characteristics in middle cerebral artery (MCA) between patients with and without hypoperfusion area, and to identify the risk factors affecting hypoperfusion area.
Background and propose
High-Resolution Vessel Wall Imaging (HR-VWI) has been developed to depict the characteristics of intracranial atherosclerotic plaque, such as plaque components, plaque burden and plaque vulnerability[1,2]. In addition, the current assumption is that the brain tissue with Tmax>6s can be the optimal threshold for the definition of critically hypoperfused tissue in patients with MCA stenosis[3,4]. The purpose of this study was to investigate the plaque characteristics in middle cerebral artery (MCA) between patients with and without hypoperfusion area, and to identify the risk factors affecting hypoperfusion area.
Methods
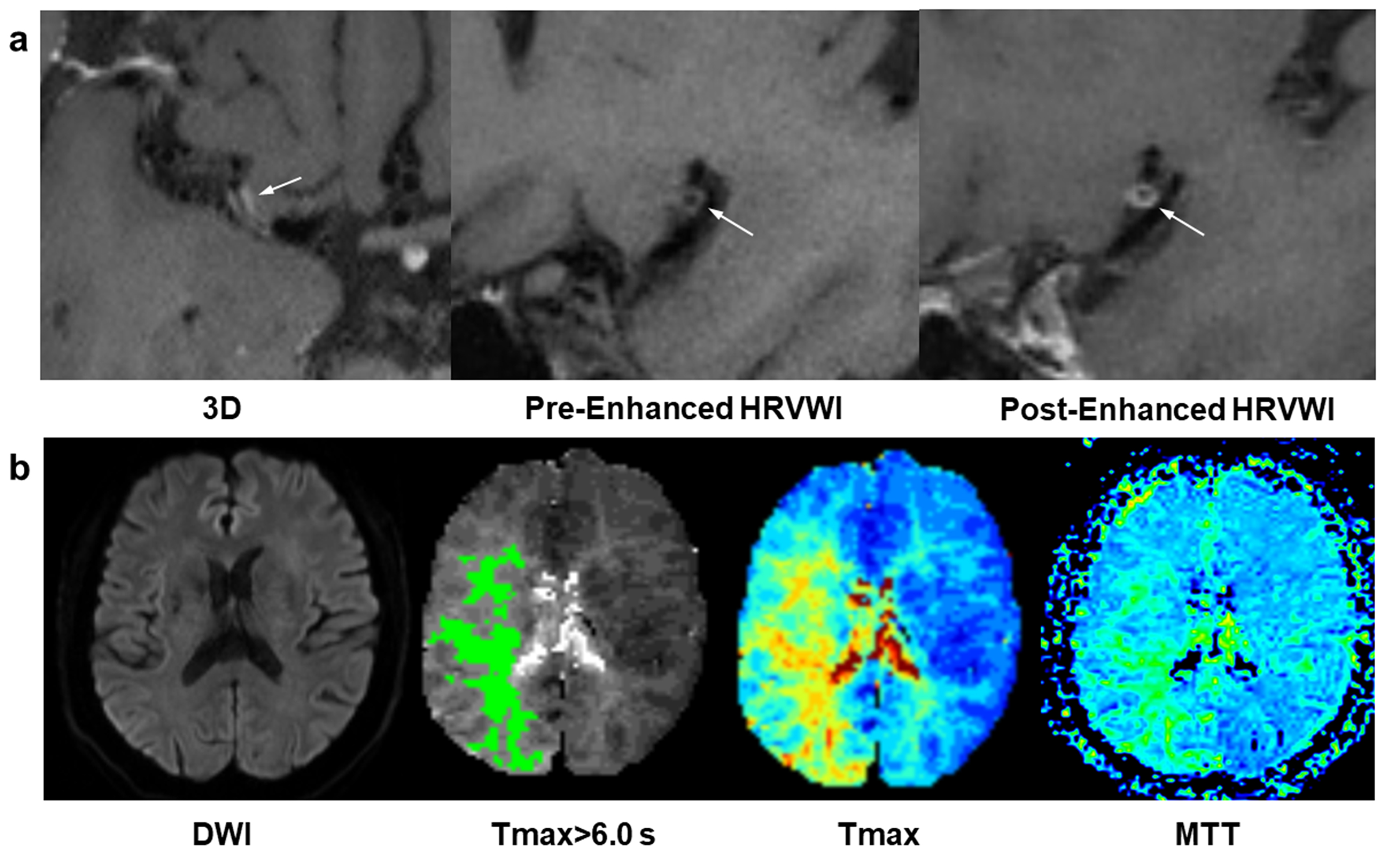
Forty-one patients (28 males; mean age: 60.2; range: 30-80 years) with over than 50% stenosis in the unilateral MCA were enrolled. Patients were scanned on 3.0 T MRI Siemens Tim Trio system (Siemens Medical Systems, Erlangen, Germany) with a 32-channel head coil. The imaging protocol incorporated the following sequences: DWI, pre-enhanced Inversion-Recovery prepared Sampling Perfection with Application-optimized Contrast using different flip angle Evolutions (IR-SPACE), post-enhanced IR-SPACE and DSC-PWI. The plaque characteristics in MCA were measured in IR-SPACE. (Figure 1) And lesion site was defined as the narrowest part of the lumen in the cross-sectional image. Three basic data were measured as follows: 1) the outer vessel wall area (OWAlesion) was recognized as the boundary between the vessel wall and cerebrospinal fluid (or meninges); 2) The inner wall in stenotic residual area was defined as the lumen area (LAlesion); 3) The wall area (WAlesion) was calculated by subtracting LAlesion from OWAlesion. The hypoperfusion volume was acquired using the RApid processing of PerfuIon and Diffusion (RAPID) system[5]. Kruskal-Wallis H test and Chi-square test were used to compare the difference of plaque characteristics between hypoperfusion group and non-hypoperfusion group. Receiver operating characteristic (ROC) curve was conducted to evaluate the area-under-the-curve (AUC) of each variable and combinations in predicting the hypoperfusion area.
Results
19 patients were enrolled in hypoperfusion group, and 22 patients in non-hypoperfusion group. The results showed that eccentric plaques were observed 9 (47.37%) in hypoperfusion group and 18 (81.82%) in non-hypoperfusion group, which had significant difference between two groups (χ2=5.381, P=0.026). (Table 1) Cases of plaques with concentric or eccentric morphology were shown in the Figure 2 and Figure 3. The AUC (95% CI) for predicating the appearance of hypoperfusion area were 0.672 (0.503-0.842) for morphology, 0.608 (0.431-0.784) for plaque length, and 0.781 (0.634-0.929) for combination of plaque length and morphology. (Figure 4) Patients with plaques enhancement had more hypoperfusion volume comparing to that without enhancement in hypoperfusion group (48.21 ml versus 5.00 ml, Z=-2.781, P=0.003).
Conclusions
The presence of concentric plaque of MCA have a higher likelihood of hypoperfusion appearance. Combination of plaque morphology and length provide the incremental contribution to predict the hypoperfusion brain tissue. Positive enhanced plaques are associated with a larger hypoperfusion volume in patients with hypoperfusion area.
Acknowledgements
The authors thank Zhiyun Wang, PhD, of Department of Neurology, Tianjin First Central Hospital for patient recruitment; Meizhu Zheng, MD, of Department of Radiology, Tianjin Third Central Hospital for statistical consultation; Jian Wang, MD, of Department of Radiology, Tianjin First Central Hospital for image acquisition.References
[1] Xu WH, Li ML, Gao S, Ni J, Zhou LX, Yao M, Peng B, Feng F, Jin ZY, Cui LY. In vivo high-resolution MR imaging of symptomatic and asymptomatic middle cerebral artery atherosclerotic stenosis. Atherosclerosis. 2010 Oct;212(2):507-11.
[2] Ryu CW, Jahng GH, Kim EJ, Choi WS, Yang DM. High resolution wall and lumen MRI of the middle cerebral arteries at 3 tesla. Cerebrovasc Dis. 2009;27(5):433-42.
[3] Lansberg MG, Straka M, Kemp S, Mlynash M, Wechsler LR, Jovin TG, Wilder MJ, Lutsep HL, Czartoski TJ, Bernstein RA, Chang CW, Warach S, Fazekas F, Inoue M, Tipirneni A, Hamilton SA, Zaharchuk G, Marks MP, Bammer R, Albers GW; DEFUSE 2 study investigators. MRI profile and response to endovascular reperfusion after stroke (DEFUSE 2): a prospective cohort study. Lancet Neurol. 2012 Oct;11(10):860-7.
[4] Calamante F, Christensen S, Desmond PM, Ostergaard L, Davis SM, Connelly A. The physiological significance of the time-to-maximum (Tmax) parameter in perfusion MRI. Stroke. 2010 Jun;41(6):1169-74.
[5] Straka M, Albers GW, Bammer R. Real-time diffusion-perfusion mismatch analysis in acute stroke. J Magn Reson Imaging. 2010 Nov;32(5):1024-37.
Figures