2940
Alteration of cerebrovascular response for COPD patients underwent non-invasive nerve stimulation treatment in nasal cavityLi Tieqiang1, Jan-Erik Juto1, Karin Sandek2, and Daniel Alamidi3
1Department of Medical Radiation and Nuclear Medicine, Karolinska university Hospital, Huddinge, Sweden, 2Capio S:t Göran, Stockholm, Sweden, 3The Royal Insititute of Technlogy, Huddinge, Sweden
Synopsis
Chronic obstructive pulmonary disease (COPD) is currently the third leading mortality cause in the world. There is neither a reliable blood biomarkers to confirm its diagnosis nor curative treatment. In this study we tested the hypothesis that the lung function and cerebrovascular responsiveness for COPD patients may be altered by a novel therapy through restoration of ANS homeostasis along with the improvement of clinical symptoms.
Introduction
Chronic obstructive pulmonary disease (COPD) is a heterogeneous lung disease characterized by chronic obstruction of lung airflow that is not fully reversible. COPD is currently the third leading mortality cause in the world. There is neither a reliable blood biomarkers to confirm its diagnosis nor curative treatment. COPD is usually associated with systemic inflammation and dysfunction of the autonomic nervous system (ANs)1,2. We have recently developed a non-invasive nerve stimulation technique through the nasal cavity, which function as a homeostasis restoration (HOMER) has been shown to have therapeutic efficacy for COPD and other chronic inflammatory diseases3,4. In this study we tested the hypothesis that the lung function and cerebrovascular responsiveness for COPD patients may be altered by the HOMER therapy through restoration of ANS homeostasis along with the improvement of clinical symptoms.Methods
Nine patients (female/male=4/5, aged 59-79 years old) clinically diagnosed as having moderate degree of COPD symptoms (grade 2-3) were recruited into the study. All patients received at least 10 HOMER treatments over a period of 3 weeks. Each treatment lasted for about 20 min (10 min for each side of the nasal cavities) as described previously. The subjects underwent clinical assessment by COPD medical expert and MRI examinations both before and within one week after the completion of the HOMER treatment. The clinical evaluations included the followings (1) quality of life according to COPD assessment test (CAT); (2) Six minutes walking test (6MWT); (3) spirometry measurements. The MRI protocol included (1) T1 mappings of the lung under air and enhanced oxygen conditions; (2) Functional imaging of the brain using a block-designed hyperoxia paradiam which lasted for 12 min consisting of 3 air breathing epochs interleaved with 3 epochs of pure oxygen breathing. Each epoch lasted 2 min. The administration was O2 accomplished through a MRI compatible facemask. All MRI data acquisition was conducted on a whole-body 3T clinical MRI scanner (Ingenia CX, Philips Medical System) equipped with a 16-channel head coil and 32-channel body array coil. A multiple flip angle UTE protocol was selected for T1-mapping of the lung5, 6. For the fMRI study of the brain a single-shot 2D GRE-EPI pulse sequence was used to acquire a 12 min time series of GRE fMRI dataset during hyperoxia paradigm described above. The main acquisition parameters for the R-fMRI datasets were the followings: 41 axial oblique slices of 3 mm thick, TR/TE=2000/30 ms, , matrix size=80x80, flip angle=75°, parallel acceleration factor=2. The MRI datasets underwent a standard preprocessing procedure7, which was performed with AFNI and FSL (http://www.fmrib.ox.ac.uk/fsl) programs with a bash wrapper shell. The first 5 timeframes in each dataset were removed to ensure signal steady state. After de-spiking, six-parameter rigid body image registration was performed for motion correction. The average volume for each motion-corrected time series was used to generate a brain mask to minimize the inclusion of the extra-cerebral tissue. Spatial normalization to the Montreal Neurological Institute (MNI) standard-space T1-weighted average structural template image was performed using a 12-parameter affine transformation and mutual-information cost function. Nuisance signal removal was performed by voxel-wise regression using 14 regressors based on the motion correction parameters, average signal of the ventricles and their 1st order derivatives. After removing baseline trend up to the third order polynomial, effective band-pass filtering was performed using low-pass filtering at 0.08 Hz. Local Gaussian smoothing up to FWHM = 4 mm was performed using an eroded gray matter mask. The correlation coefficient (CC)for the fMRI time course and hyperoxia paradigm was computed voxel wise. The paired t-test was used to assess the CC alteration before and after HOMER treatments. Statistical significance was assessed with an initial cluster-forming voxel-wise threshold of p<0.001 and model-free randomized permutation simulation was used to estimate the corrected family-wise error rate (FWER) for the clusters.Results
As shown in Fig. 1, 8/9 patients had improved CAT score following 10 HOMER treatments in 3 weeks and the average improvement in CAT score was 29%. 6/9 patients had increased talking distance in 6MWT evaluation. The average increase was 4.5% corresponding to 18 meters. May inhance the CBF response to hyperoxia. As shown in Fig. 2, only very few limited brain regions including the precuneus, Para hippocampal gyrus, and lentiform nucleus had altered cerebrovascular responsiveness to hyperoxia. As illustrated in Fig. 3, almost all subjects (except for one) demonstrated change from nearly non-responsiveness to vasodilation to hyperoxia instead of vasoconstriction.Conclusion
The preliminary results from this pilot study indicate that HOMER treatment that has clinical efficacy may alter cerebrovascular responsiveness to hyperoxia for COPD patients.Acknowledgements
No acknowledgement found.References
1. Bernardo, A.F., L.C. Vanderlei, and D.M. Garner, HRV Analysis: A Clinical and Diagnostic Tool in Chronic Obstructive Pulmonary Disease. Int Sch Res Notices, 2014. 2014: p. 673232. 2. Chhabra, S.K., et al., Cardiac Sympathetic Dominance and Systemic Inflammation in COPD. COPD, 2015. 12(5): p. 552-9. 3. Li, T.Q., et al., Resting-state fMRI study of acute migraine treatment with kinetic oscillation stimulation in nasal cavity. Neuroimage Clin, 2016. 12: p. 451-9. 4. Juto, J.E. and R. Hallin, Kinetic oscillation stimulation as treatment of acute migraine. A randomized, controlled pilot study. Headache, 2015. 55: p. 11. 5. Alamidi, D.F., et al., T1 Relaxation Time in Lungs of Asymptomatic Smokers. PLoS One, 2016. 11(3): p. e0149760. 6. Alamidi, D.F., et al., COPD Patients Have Short Lung Magnetic Resonance T1 Relaxation Time. COPD, 2016. 13(2): p. 153-9. 7. Wang, Y. and T.Q. Li, Analysis of whole-brain resting-state FMRI data using hierarchical clustering approach. PLoS One, 2013. 8(10): p. e76315.Figures

Bar graph of
the 6MWT results for individual patient before and after completion of the 10
HOMER treatments (a). Bar graph of the CAT scores for individual patient before
and after completion of the HOMER treatments (b). The scatter plot of the
changes in CAT scores versus the changes in 6MWT results (c).
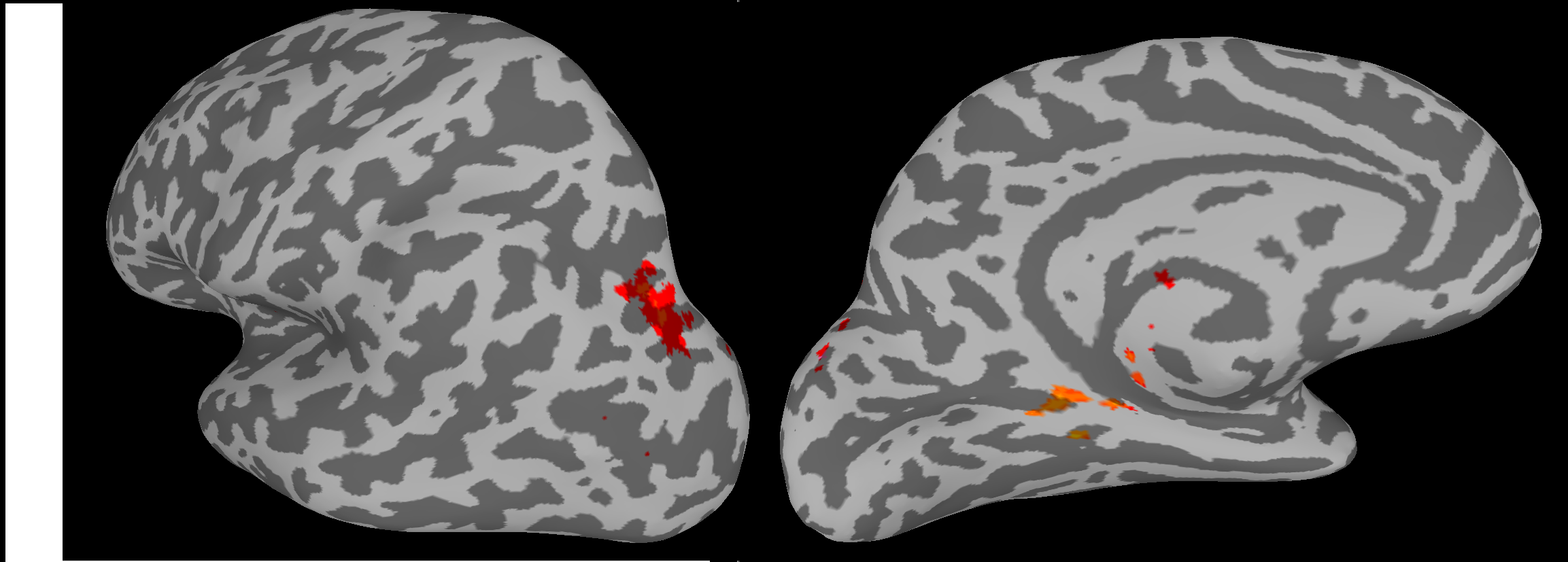
Paired
t-test of results of the fMRI signal responses to hyperoxia paradiam before and
after the HOMER treatment. The colored clusters depict the brain regions with
significant alteration (p< 0.05) in cerebrovascular responsiveness to hyperoxia 100%
O2) overlaid on to the inflated MNI model.

Plot of the
average correlation coefficient between the fMRI signal time course and the
hyoeroxia paradigm for brain regions with significant alteration (p< 0.05)
in cerebrovascular responsiveness to hyperoxia (the clusters depicted in Fig.
2). The results for both the individual patient (shown in circles) and cohort
(box plot) are depicted.