2938
Dilatation, Proliferation, and Abnormal Anastomosis of Lenticulostriate Arteries on Whole-Brain Vessel Wall Imaging as a Predictor of Hemorrhage in Patients with Moyamoya Disease1Xuanwu Hospital, Capital Medical University, Beijing, China, 2307 Hospital of Chinese People's Liberation Army, Beijing, China, 3Cedars Sinai Medical Center, Los Angeles, CA, United States
Synopsis
In this
study, we explored distinct branching pattern of lenticulostriate arteries
(LSAs) in moyamoya disease (MMD) and identified collateral features of
hemorrhagic MMD, using whole-brain vessel wall imaging (WB-VWI). Results showed
that patients with MMD more frequently presented with dilated and proliferated LSA
branches than patients with atherosclerotic moyamoya syndrome. In patients with
MMD, type 3 LSA pattern (dilatation and proliferation of LSA branches with abnormal
anastomosis) was associated with hemorrhagic events and vanished middle
cerebral artery. These findings suggest that WB-VWI can provide complementary
information of abnormal moyamoya vessels and facilitate to predict hemorrhage
in MMD.
Background and Purpose
Intracranial hemorrhage is one of the most serious complications in patients with moyamoya disease (MMD) that worsens functional outcome and increases the mortality rate, which can be detected in about half of adult patients[1]. Dilated, fragile collateral vessels in MMD is known to be associated with hemorrhagic events[2,3]. Nevertheless, it is unable to reveal the position relation between hemorrhage and abnormal perforating arteries on digital subtraction angiography (DSA). A previous study has used black-blood magnetic resonance angiography to visualize periventricular collaterals in MMD and found their relationship with microbleeds[4]. However, the correlation between collaterals on MRI and hemorrhage has not been systematically studied. Our recent study has demonstrated the feasibility of whole-brain vessel wall imaging (WB-VWI) in depicting lenticulostriate arteries (LSAs)[5]. Thus, the aim of the present study was to investigate branching pattern of LSAs in MMD and atherosclerotic moyamoya syndrome (A-MMS), and to explore the relationship between abnormal changes of perforating arteries and hemorrhagic events, using WB-VWI.Material and methods
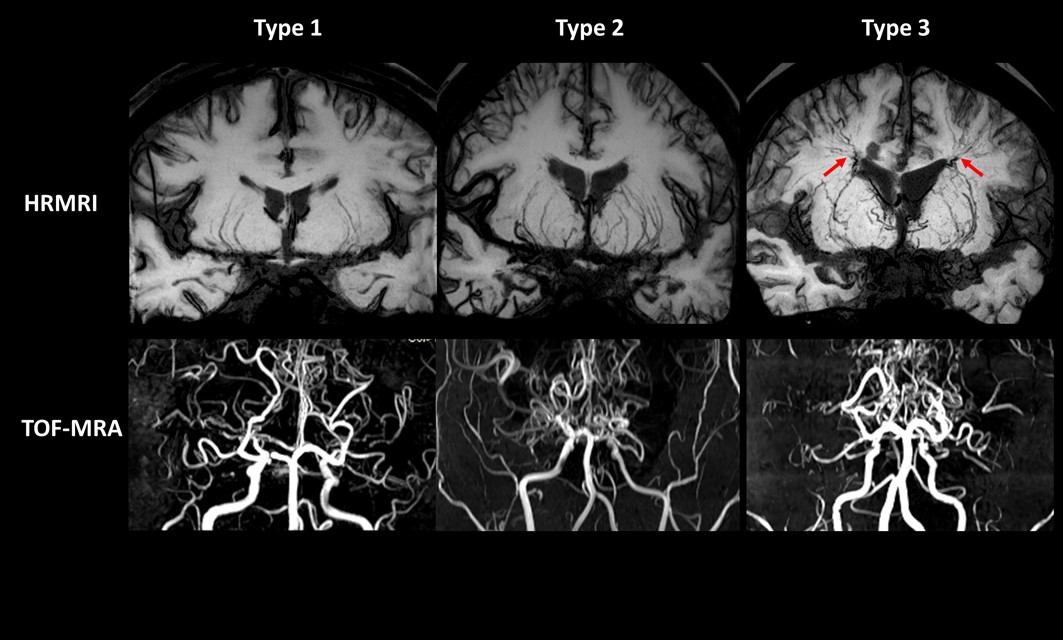
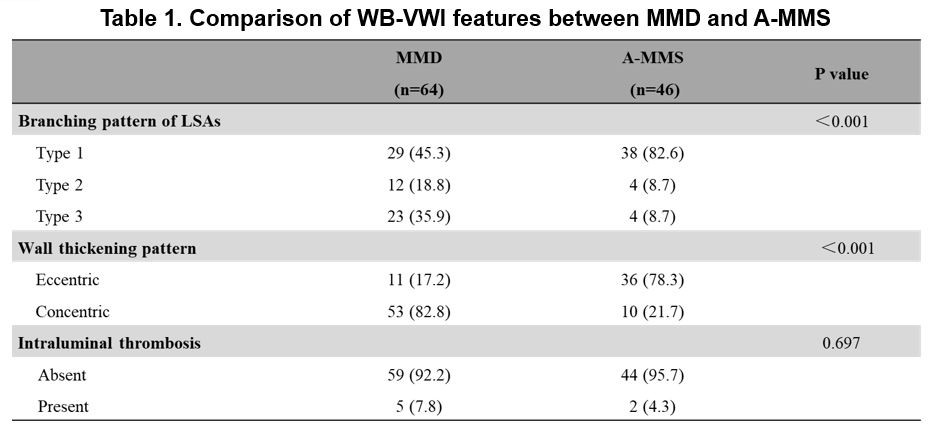
Adult patients with MMD and A-MMS were prospectively enrolled and underwent WB-VWI exams. WB-VWI was performed on a MAGNETOM Verio 3T MR system (Siemens Healthcare, Erlangen, Germany) with 3D T1-weighted and T2-weighted whole-brain vessel wall sequences: TR/TE = 900/15 ms (T1-weighted imaging) and 1800/177 ms (T2-weighted imaging); field of view = 170×170 mm2; 240 slices with slice thickness of 0.53 mm; voxel size = 0.53×0.53×0.53 mm3; and scan time = 8 min. Branching patterns of LSA in each affected hemisphere were defined as: type 1 = no dilation or proliferation, type 2 = dilation and proliferation without anastomosis, type 3 = dilation and proliferation with anastomosis (Figure 1). Vessel wall thickening pattern (eccentric and concentric), morphology of occluded middle cerebral artery (MCA) (plugged and vanished), and intraluminal thrombosis (absent and present) were also evaluated. The right and left hemispheres in each MMD patient were individually classified as symptomless, TIA and headache, infarction, or hemorrhage. LSA pattern, vessel wall thickening pattern, and intraluminal thrombosis were compared using Chi-square tests between MMD and A-MMS. Associations between LSA pattern and symptoms, as well as morphology of occluded MCA in MMD were assessed using Chi-square tests.Results
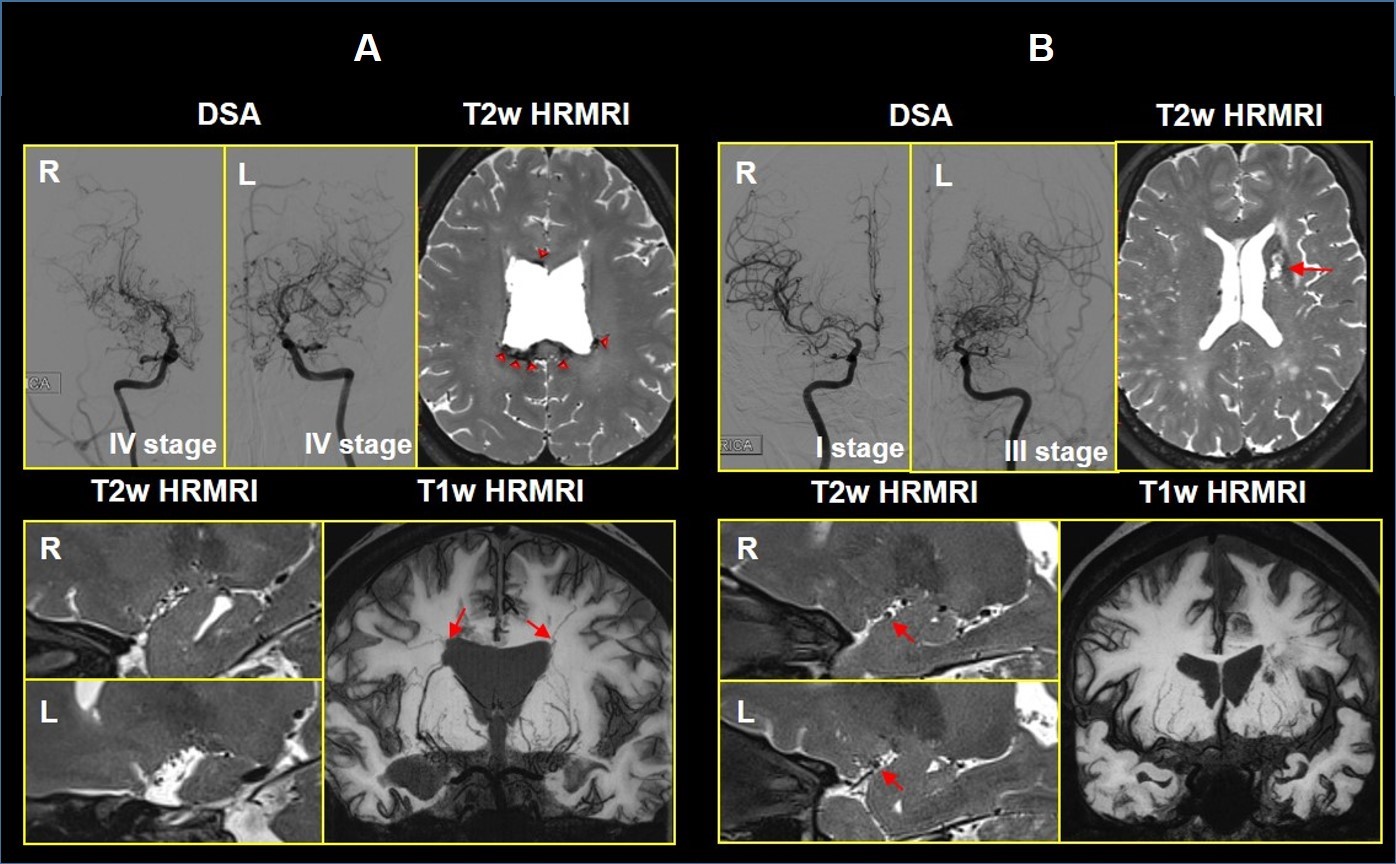
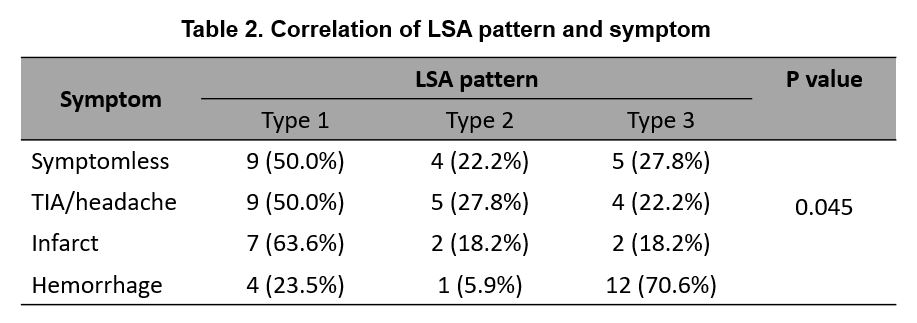
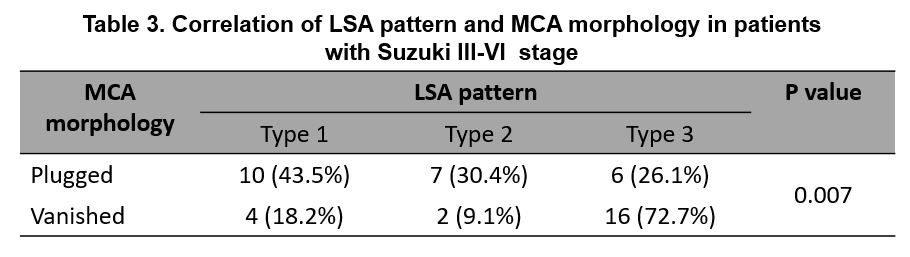
Fifty-five patients (110 hemispheres) were enrolled, including 32 (64 hemispheres) MMD and 23 (46 hemispheres) A-MMS. Dilated and proliferated LSA branches (type 2 and 3) were likely (P < 0.001) to be detected in patients with MMD (54.7%) than A-MMS (17.4%) (Figure 1, Table 1). Concentric wall thickening was more frequently observed in MMD than A-MMS (82.8% versus 21.7%, P < 0.001) (Table 1). In 64 hemispheres of MMD, 18 sides were symptomless, 18 sides were TIA/headache, 11 sides were infarction, and 17 sides were hemorrhage (intraventricular hemorrhage in 12, intraparenchymal hemorrhage in 4, subarachnoid hemorrhage in 1). Type 3 LSA pattern was associated with hemorrhagic events (P = 0.045) (Figure 2, Table 2). Furthermore, in MMD patients with Suzuki stage Ⅲ~Ⅳ, type 3 LSA pattern correlated with vanished MCA (P = 0.007) (Figure 2, Table 3).Discussion
DSA was commonly used in previous studies of moyamoya vessels. However, most of the collaterals, and the position relation between hemorrhage and abnormal perforating arteries have barely been identified through DSA. In our study, we used a novel 3D whole-brain vessel wall MRI technique, which may provide the information of both perforating artery morphology and the anastomosis site. In our study, we found that dilated/proliferated LSA branches were frequently presented in MMD, which is in line with their pathogenesis and natural course. In MMD, a very slow and progressive steno-occlusive process in the MCA may induce the formation of unusual collateral vessels, such as the significant dilation of the perforating arteries[6]. On the contrary, atherosclerotic plaques blocking the orifice of LSA branches may cause occlusion of these small arteries[7]. Our results also showed that dilated/proliferated LSA branches with anastomosis was associated with hemorrhagic events. Besides, 70.6% (12/17) of hemorrhagic hemispheres were intraventricular hemorrhage, and all the abnormal anastomosis sites were located in periventricular area. Furthermore, dilated/proliferated LSA branches with anastomosis also correlated with vanished MCA, which may be because an altered hemodynamic load from the MCA to the collateral vessels induces atrophic remodeling of the MCA trunk.Conclusion
In MMD, dilation, proliferation, and anastomosis of LSA branches are a predictor of hemorrhagic events. WB-VWI can provide complementary information of abnormal moyamoya vessels, which might facilitate future optimal grading and classifcation of moyamoya vessels.Acknowledgements
No acknowledgement found.References
[1] Kuroda S, Houkin K. Moyamoya disease: current concepts and future perspectives. Lancet Neurology. 2008, 7(11):1056-1066.
[2] Iwama T, Morimoto M, Hashimoto N, et al. Mechanism of intracranial rebleeding in moyamoya disease. Clinical Neurology & Neurosurgery, 1997, 99(10):S187–S190.
[3] Morioka M, Hamada J, Kawano T, et al. Angiographic dilatation and branch extension of the anterior choroidal and posterior communicating arteries are predictors of hemorrhage in adult moyamoya patients. Stroke, 2003, 34(1):90-95.
[4] Funaki T, Fushimi Y, Takahashi J C, et al. Visualization of Periventricular Collaterals in Moyamoya Disease with Flow-sensitive Black-blood Magnetic Resonance Angiography: Preliminary Experience. Neurologia medico-chirurgica, 2015, 55(3):204-209.
[5] Zhang Z, Fan Z, Kong Q, et al. Visualization of the lenticulostriate arteries at 3T using black-blood T1-weighted intracranial vessel wall imaging: comparison with 7T TOF-MRA. European Radiology, 2018.
[6] Cho HJ, Song DB, Choi HY, et al. Lenticulostriate-medullary artery anastomoses in moyamoya disease. Neurology, 2007, 68(15):E21.
[7] Bang OY, Heo JH, Kim JY, et al. Middle cerebral artery stenosis is a major clinical determinant in striatocapsular small, deep infarction. Archives of neurology 2002, 59(2):259-263.
Figures