2935
Investigation of Whole Brain Coverage 4D-MR Angiography with Pseudo-Continuous Arterial Spin Labeling Combined with CENTRA-Keyhole and View-sharing (4D-PACK) Accelerated by Compressed-SENSE1Philips Japan, Ltd., Tokyo, Japan, 2Department of Clinical Radiology, Graduate School of Medical Sciences, Kyushu University, Kyushu University, Fukuoka, Japan, 3Division of Radiology, Department of Medical Technology, Kyushu University, Fukuoka, Japan, 4Asia Pacific, Philips Healthcare, Tokyo, Japan
Synopsis
Four dimensional (4D) MR Angiography based on Pseudo-Continuous Arterial Spin Labeling (pCASL) combined with CENTRA-Keyhole and View-sharing (4D-PACK) was accelerated for whole brain 4D-MRA. Compressed-Sensing combined with Sensitivity Encoding (Compressed-SENSE) was used and we demonstrated whole brain 4D-PACK accelerated with Compressed-SENSE. It provides comparable peripheral and posterior cerebral artery visualizations compared with conventional 4D-PACK which has limited anatomical coverage. Validity of whole brain 4D-MRA is suggested using Compressed-SENSE combined 4D-PACK.
Purpose
Four dimensional (4D) MR Angiography based on Pseudo-Continuous Arterial Spin Labeling (pCASL) combined with CENTRA-Keyhole and View-sharing (4D-PACK) has been proposed1,2. Acquisition times are reduced by using Keyhole and View-sharing. High flow visualization capability intracranially was demonstrated1,2. However, whole brain was not covered due to scan time limitation. To increase scan coverage while keeping the same scan time, additional scan acceleration is required, e.g. by increasing Sensitivity Encoding (SENSE) factor. In the case of increasing SENSE factor, however, geometry related noise amplification can become problematic. Recently, Compressed Sensing combined with SENSE (Compressed-SENSE) has shown its scan acceleration ability. In this study, we combined Compressed-SENSE with 4D-PACK for whole brain application and assessed its flow visualization ability compared with conventional 4D-PACK.Methods
Magnetic Resonance (MR) Experiments
4D-PACK scheme was implemented on a 3.0T Ingenia scanner (Philips, Best, The Netherlands). Flow visualization was compared between conventional 4D-PACK covering 8cm slab thickness (4DP) and 4D-PACK combined with Compressed-SENSE covering 12cm slab thickness for whole brain (4DP-WB). Five healthy subjects (mean age 36.4 years) were examined with 4DP and 4DP-WB. Sequence parameters used in this study are shown in Figure 1. Informed consent required by the Institutional Review Board was obtained.
Validation of flow visualization
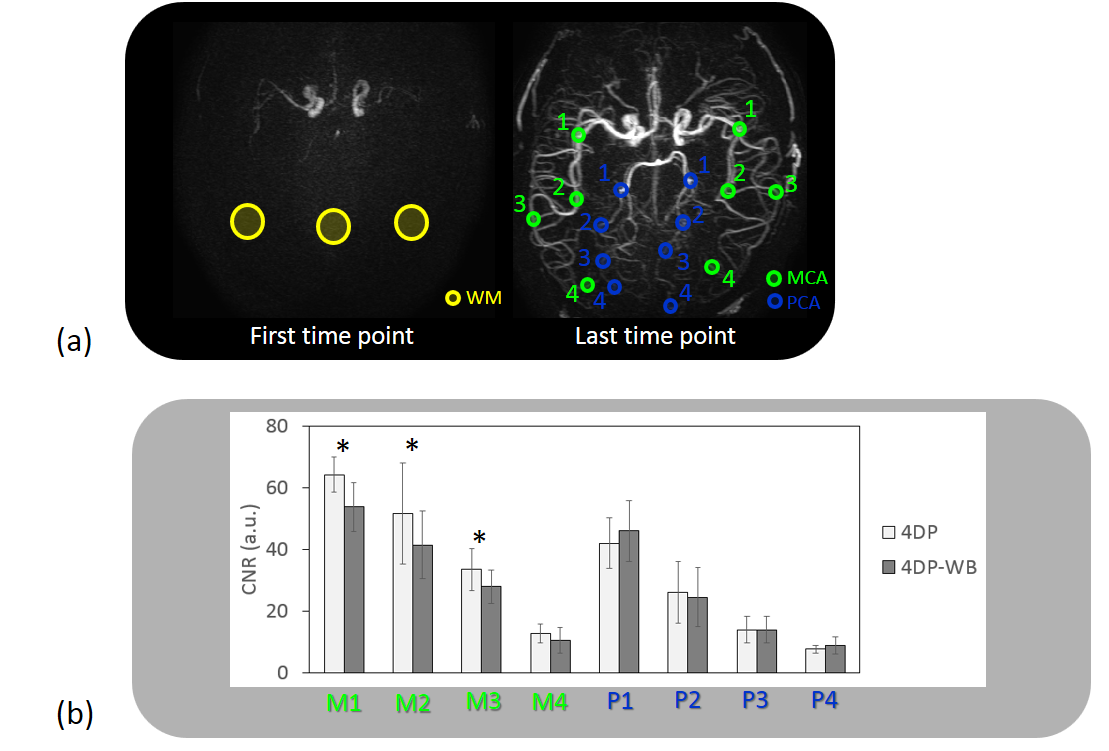
For image evaluation, 80-mm axial slab maximum intensity projection images generated with same positioning between 4DP and 4DP-WB were used. For the assessment of artery visualization, circular regions of interest (ROI) were selected from the white matter (WM), middle cerebral artery (MCA) and posterior cerebral artery (PCA). Four ROIs for MCA (M1, M2, M3, M4) and PCA (P1, P2, P3, P4) were placed from proximal to peripheral in left and right side. The contrast-to-noise ratio (CNR) between artery and WM was measured using the following equation:
CNR = (bloodmax–WMave)/WMSD.
Here, bloodmax is the maximum signal in all ROIs over the acquired timepoints. WMave and WMSD are the average signal and standard deviation, respectively, in the WM ROI. Averaged CNR between left and right side for each segment was calculated for the assessment. The paired T-test was used in the statistical analysis and p<0.05 was considered statistically significant.
Results and Discussion
Representative images 4D-MRA images from 4DP and 4DP-WB are shown in Figure 2 and 3. The images obtained by 4DP-WB exhibit peripheral artery visualization that is not covered by 4DP.
The average CNRs in each segment are shown in Figure 4. The CNRs in 4DP were significantly higher in segment M1, M2 and M3 compared with 4D-WB. On the other hand, there were no significant differences in CNRs in M4 and all PCA segments.
In general, geometry factor in SENSE locally rises in the middle part of the FOV. However, in Compressed-SENSE, as optimized random sampling and iterative reconstruction including denoising is used, localized noise amplifications can be reduced. This could explain why no CNR differences were observed in all PCA segments.
It is clinically critical to visualize the peripheral arteries. However, in 4D-PACK this visualization is jeopardized as flow signal is decreased with longer transit time compared to proximal region. Therefore, the fact that there are no CNR differences in peripheral artery segments, M4 and P4, suggests validity of 4DP-WB in clinical use.
Conclusion
Whole brain 4D-PACK using C-SENSE provides comparable peripheral and PCA visualizations. The feasability of whole brain 4D-MRA is suggested using Compressed-SENSE combined with 4D-PACK.Acknowledgements
No acknowledgement found.References
1. Osamu T et al. Eur Radiol. 2018 Nov;28(11):4871-4881
2. Obara M et al. Magn Reson Med. 2018 Aug;80(2):719-725
Figures



Figure 3. Representative images of 4DP and 4DP-WB in sagital view.