2929
Measuring cerebrovascular reactivity without gas challenge: a real-time phase-contrast MRI approach1Department of Radiology, Johns Hopkins University School of Medicine, Baltimore, MD, United States, 2Biomedizinische NMR, MPI fuer Biophysikalische Chemie, Goettingen, Germany
Synopsis
Cerebrovascular reactivity (CVR) is typically measured from changes in cerebral perfusion responsive to a hypercapnic gas challenge. Recent attempts to measure CVR using resting-state BOLD fMRI without gas challenge have utilized spontaneous fluctuations in breathing patterns. Since BOLD signal is an indirect measure of cerebral perfusion, a technique that enables cerebral blood flow (CBF)-based CVR under free-breathing conditions is highly desirable. Here, we used a real-time (17 fr/s) PC MRI to measure CBF-based CVR in the resting-state. We evaluated the feasibility of this new approach, and compared it with real-time PC MRI with gas-inhalation, and regular PC MRI with gas-inhalation.
INTRODUCTION
Cerebrovascular reactivity (CVR), an important index of a blood vessel’s dilatory function in the brain, is typically measured from changes in cerebral perfusion responsive to a hypercapnic gas challenge1. Because hypercapnic gas challenges require breathing apparatus and substantial subject cooperation, they are not widely used in clinical settings. Recent attempts to measure CVR using resting-state BOLD (rs-BOLD) fMRI without gas challenge have utilized spontaneous fluctuations in breathing patterns (thereby end-tidal CO2 (EtCO2))2-4. However, BOLD fMRI provides only an indirect measure of cerebral perfusion, so BOLD-based CVR can be confounded by hemodynamic and metabolic parameters including hematocrit, cerebral blood volume and oxygen metabolism. Therefore, a technique that enables cerebral blood flow (CBF)-based CVR under free-breathing conditions is highly desirable. Standard CBF techniques–arterial spin labeling (ASL)5 and phase-contrast (PC) MRI6–are too slow (~10s per image) to capture the dynamic changes in EtCO2 during spontaneous breathing. Therefore, we used a real-time (17 fr/s) PC MRI to measure CBF dynamically in the resting-state to obtain CBF-based CVR without gas-inhalation. We evaluated the feasibility of real-time PC MRI without gas-inhalation, and compared the results with two alternative techniques: real-time PC MRI with gas-inhalation, and regular PC MRI with gas-inhalation.METHODS
Study design: Five healthy subjects (age 22.0±3.6 yr) were scanned on a Siemens 3T Prisma scanner using three CVR protocols wherein EtCO2 was recorded using a capnograph: 1) a 7min real-time PC MRI without gas-inhalation; 2) a 3min real-time PC with CO2 inhalation; and 3) a 3min regular PC MRI with CO2 inhalation (Figure 1).
CVR scans: The real-time PC MRI uses highly undersampled radial FLASH acquisitions with regularized nonlinear inversion reconstruction to achieve fast imaging7. Imaging parameters of the real-time PC were: 200x200x5mm3 field-of-view; 0.39x0.39x5mm3 spatial resolution; and 59.3ms temporal resolution. Regular PC MRI was performed with the same spatial resolution, 5 averages and 1min/scan. Encoding velocity (Venc) of 60cm/s and 90cm/s were used with room air and hypercapnia (5% CO2), respectively, to ensure adequate signal-to-noise to measure low flow velocity at the vessel edge and account for hypercapnia-induced velocity increase. All PC scans used axial slices positioned at 10mm above the sinus confluence, to target CBF in the superior sagittal sinus (SSS).
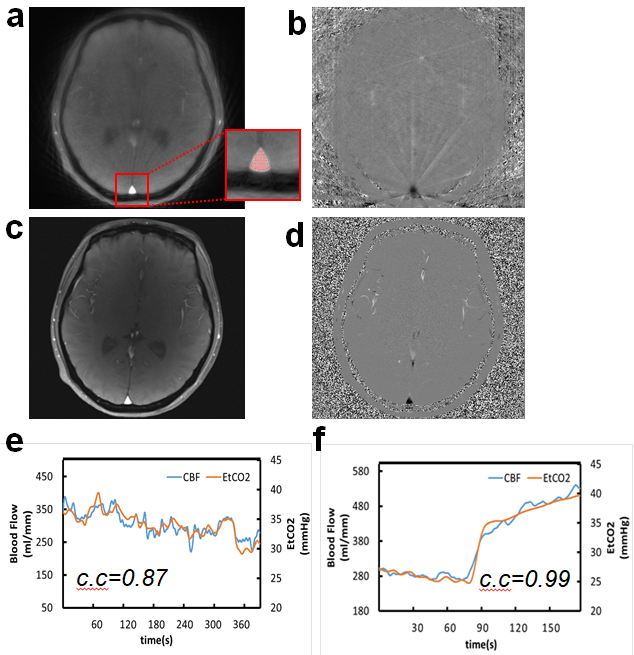
Data analysis: The SSS-ROI was automatically selected on the anatomic image for each dynamic scan using a voxel intensity-based seed-growing algorithm (Figure 2a and insert). Integration of the flow velocity from the phase image over the area of SSS-ROI yielded CBF for each dynamic. The CBF time course from real-time PC was low-pass filtered to 0.1Hz to remove the cardiac and respiratory variations, and then fed into a linear regression with EtCO2 time course to calculate CVR in the units of %ΔCBF/mmHg. CVR was calculated using standard methods of analysis for the regular PC scans1,6.
RESULTS and DISCUSSION
Figure 2a-d show typical real-time and regular PC images from a subject. Compared to the regular PC, the real-time PC images were not as well-resolved and showed some streaking artifacts due to the under-sampling, which may add noise to CBF quantification. Figure 2e-f show the real-time CBF and corresponding EtCO2 time courses during resting-state and CO2 inhalation.
Figure 3 compares baseline CBF, baseline EtCO2 and EtCO2 change (ΔEtCO2) in the three CVR scans averaged over the 5 subjects. There were no significant differences between baseline CBF and EtCO2 among the three scans (p>0.2, paired t-test), suggesting 1) real-time PC can provide the same CBF quantification as regular PC, despite the image blur and streaking artifacts observed, and 2) baseline physiological conditions were comparable across the three CVR scans, enabling comparison of the different CVR methodologies. As expected, the EtCO2 change is smaller in resting-state scan than with CO2 inhalation.
The CVR values from the real-time PC resting-state scan, the real-time PC CO2 inhalation scan and the regular PC CO2 inhalation scan were 3.7±1.3, 3.8±1.2 and 3.6±0.7 %ΔCBF/mmHg, respectively. No significant difference was found among the three CVR scans (Figure 4, p>0.4), suggesting that real-time PC can provide CBF-based CVR measurements reliably both with and without CO2 inhalation.
CONCLUSION
In the present study, we demonstrated that real-time phase-contrast MRI approach can measure CBF-based CVR based on just the dynamic CBF changes associated with spontaneous fluctuations in free-breathing, without requiring specialized gas-inhalation devices and complex patient protocols. CVR values obtained by this approach are indistinguishable from conventional CO2 inhalation methods. This new CVR approach should facilitate studies in conditions involving global vascular degeneration, such as normal aging, small vessel disease and multiple sclerosis.Acknowledgements
Grant support: NIH R01 EB007829.References
1. Liu P, De Vis JB, Lu H. Cerebrovascular reactivity (CVR) MRI with CO2 challenge: A technical review. Neuroimage. 2018;doi: 10.1016/j.neuroimage.2018.03.047.
2. Golestani AM, Chang C, Kwinta JB, Khatamian YB, Chen JJ. Mapping the end-tidal CO2 response function in the resting-state BOLD fMRI signal: spatial specificity, test-retest reliability and effect of fMRI sampling rate. Neuroimage. 2015;104: 266-277.
3. Jahanian H, Christen T, Moseley ME, Pajewski NM, Wright CB, Tamura MK, Zaharchuk G, Group, S.S.R. Measuring vascular reactivity with resting-state blood oxygenation level-dependent (BOLD) signal fluctuations: A potential alternative to the breath-holding challenge? J Cereb Blood Flow Metab. 2017;37:2526-2538.
4. Liu P, Li Y, Pinho M, Park DC, Welch BG, Lu H. Cerebrovascular reactivity mapping without gas challenges. Neuroimage. 2017;146:320-326.
5. Gauthier CJ, Madjar C, Desjardins-Crépeau L, Bellec P, Bherer L, Hoge RD. Age dependence of hemodynamic response characteristics in human functional magnetic resonance imaging. Neurobiol Aging. 2013;34(5):1469-85.
6. Xu F, Uh J, Brier MR, Hart J Jr, Yezhuvath US, Gu H, Yang Y, Lu H. The influence of carbon dioxide on brain activity and metabolism in conscious humans. Cereb Cortex. 2011;21(6):1426-34.
7. Untenberger M, Tan Z, Voit D, Joseph AA, Roeloffs V, Merboldt KD, Schaetz S, Frahm J. Advances in real-time phase-contrast flow MRI using asymmetric radial gradient echoes. Magn Reson Med. 2016;75(5):1901-8.
Figures