2925
The Acute Effects of Cigarette Smoking on Brain Oxygenation and Perfusion Measured by Multi-Parametric Quantitative BOLD and Arterial Spin Labeling MRI: Preliminary Results1Computer Assisted Clincial Medicine, Heidelberg University, Mannheim, Germany, 2Department of Addictive Behavior and Addiction Medicine, Central Institute of Mental Health, Heidelberg University, Mannheim, Germany
Synopsis
The effects of smoking on human brain hemodynamics have been investigated for many years, but no real consensus was found. In this study, the acute effects of cigarette smoking on the cerebral blood flow, oxygen extraction fraction and cerebral metabolic rate of oxygen are measured with a multi-parametric quantitative BOLD approach. So far, no significant difference between pre- and post-smoking was found. However, the number of subjects will be increased from 5 to 20 in the course of this ongoing study.
Introduction
The acute effects of cigarette smoking on human brain hemodynamics have been investigated for many years using several imaging modalities, such as positron emission tomography,1 single photon emission tomography2 and magnetic resonance angiography.3 Yet, the reported results vary considerably among the studies and, thus, there is no real consensus. Here, we investigated the impact of acute nicotine administration on the hemodynamic parameters cerebral blood flow (CBF), oxygen extraction fraction (OEF) and cerebral metabolic rate of oxygen (CMRO2) measured with MRI using a multi-parametric quantitative BOLD approach.Methods
To date, 5 (male) out of 20 chronic smokers were recruited for this ongoing study, which was approved by the local ethics committee. All participants were asked to refrain from smoking at least 8 hours prior to the measurement and their smoking status was determined with a carbon monoxide breath test. 2D multi-gradient echo (mGRE), 2D multi-spin echo (mSE), 2D-EPI pseudo-continuous arterial spin labelling (pCASL) and T1-weighted MPRAGE data was acquired on a clinical 3T Magnetom TRIO scanner using a 32-channel head-coil (Siemens Healthineers, Erlangen, Germany). The parameters for mGRE were: TR/TE1/ΔTE=2650/4.5/5.5ms, 12 echoes, resolution 1.7x1.7x1.5mm3 with 20% slice gap, matrix size=128x96x66 and for mSE: TR/TE1/ΔTE=2650/13.1/13.1ms, 12 echoes, resolution=2x2x2mm3 with 20% slice gap, matrix size=128x96x45. The pCASL parameters were: TR/TE=5000/16ms, resolution 3x3x3mm3 with 20% slice gap, matrix size=80x80x28, 48 averages, post-label delay=1500ms, label duration=1500ms and the labelling plane was placed perpendicular to the internal carotid artery roughly 80mm below the anterior-posterior-commissure line. After scanning, the subjects took a break of 15 minutes and smoked one cigarette before all measurements were repeated once more. R2* and R2 values including a noise offset were fitted to the mGRE and mSE magnitude data respectively. CBF in mL/100g/min was estimated from the pCASL data according to the white paper4 with the deoxygenated blood volume DBV in mL/100g given by the literature5,6: DBV=0.77*2.1*CBF0.32. The MPRAGE data was segmented into gray matter (GM), white matter (WM) and cerebrospinal fluid (CSF) and all data sets were registered to the pre-smoking mGRE contrast using SPM12 (Wellcome Trust Centre for Neuroimaging, London, UK). OEF and CMRO2 in µmol/100g/min were calculated as $$\text{OEF}= \frac{3}{4πγΒ_0} \cdot \frac{R_2^*-R_2}{\text{DBV}} \cdot \frac{1}{Δχ_{\text{do}} \cdot \text{Hct}}$$ $$\text{CMRO2}= \text{OEF} \cdot \text{CBF} \cdot [\text{H}]_\text{a}$$ with the haematocrit $$$\text{Hct}=0.357$$$, susceptibility difference between fully oxy- and deoxygenated blood $$$Δχ_\text{do}=0.27\text{ppm}$$$ and the heme molar concentration $$$[\text{H}]_\text{a}=7.377\text{μmol/ml}$$$ for an arterial oxygen saturation of $$$\text{Y}_\text{a}=0.98$$$. Inter-subject means of OEF, CBF and CMRO2 were calculated in GM, WM and GM+WM for both pre- and post-smoking state and compared using two-tailed Student’s t-tests assuming significant differences for p<0.05.Results
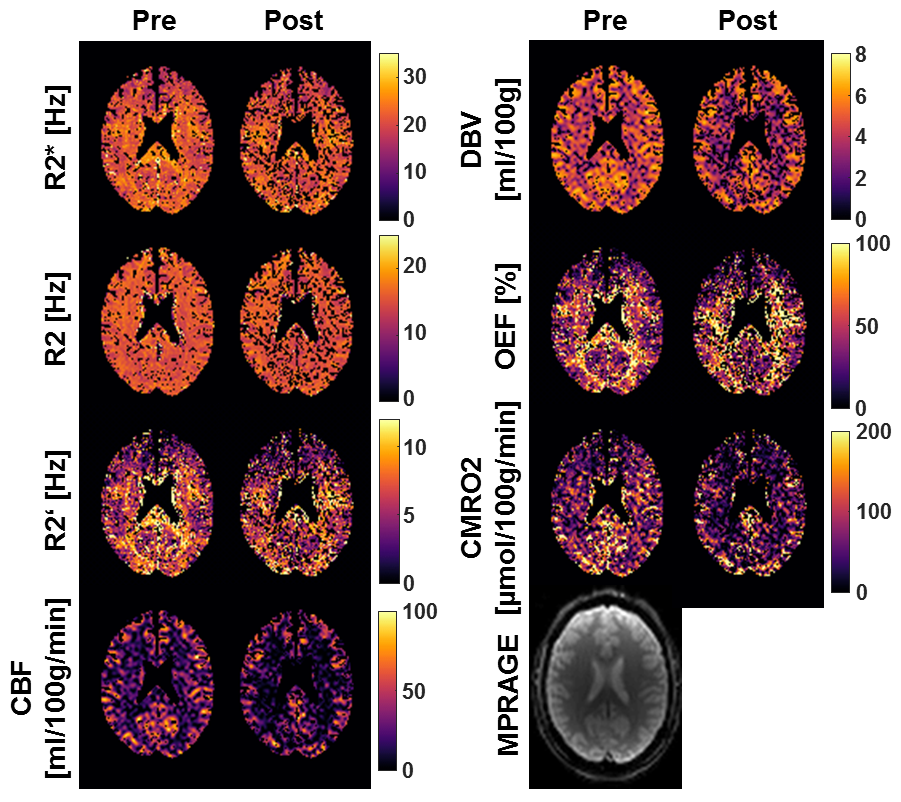
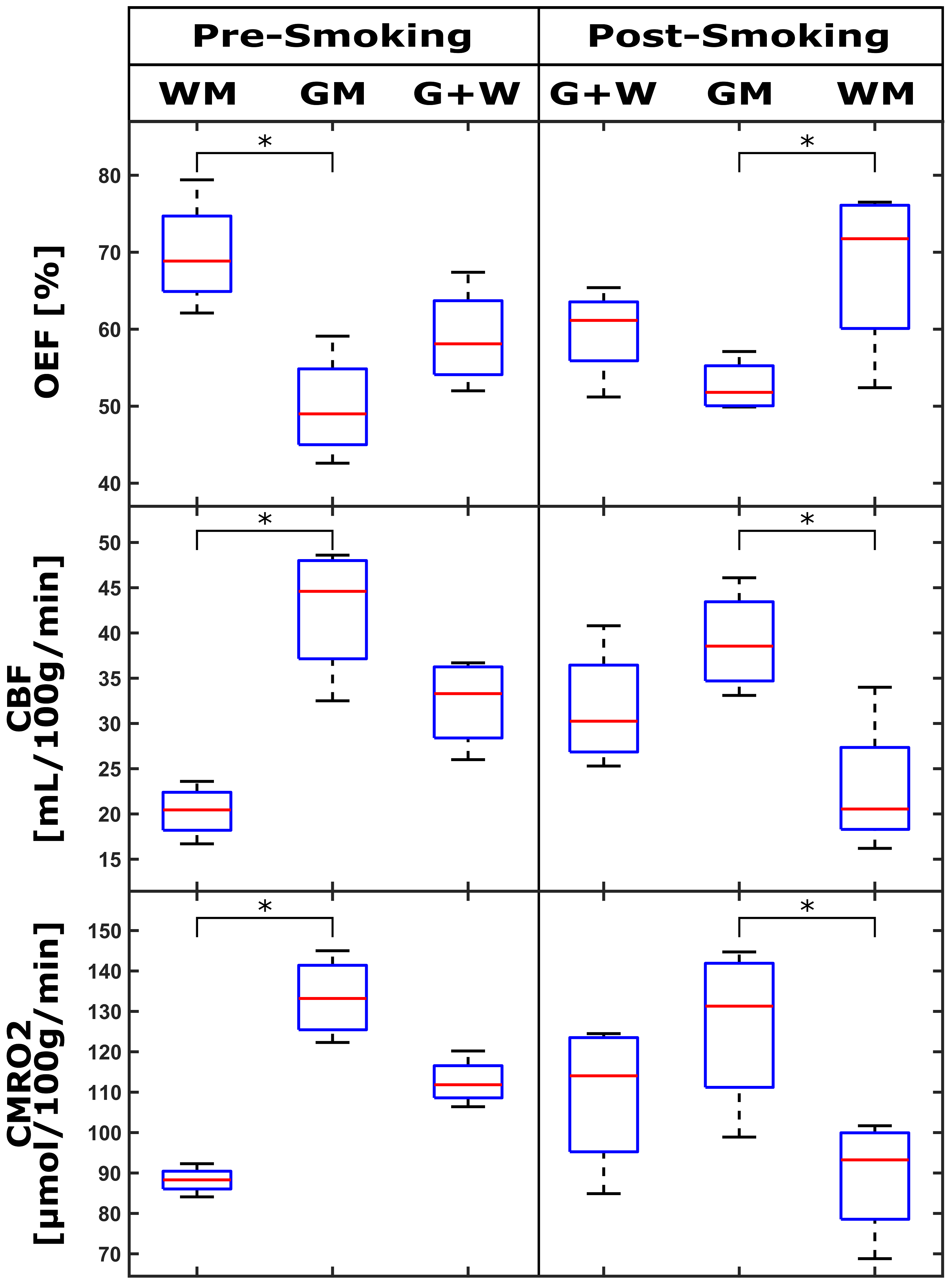
Figure 1 depicts a representative slice of the R2*, R2, R2’= R2*- R2, CBF, DBV, OEF and CMRO2 maps for the pre- and post-smoking state of a single subject. Figure 2 shows boxplots of the averaged OEF, CBF and CMRO2 within WM, GM and the combination of both for all the subjects in pre- and post-smoking state. No significant difference was found for OEF, CBF and CMRO2 in the three tissue categories between pre- and post-smoking state. All three parameters showed significant GM-WM contrast both pre- and post-smoking.Discussion
In this study, no significant change in OEF, CBF or CMRO2 was found in the brain of smokers before and after acute nicotine administration. This is partly in agreement with previous studies;7 however, no final conclusions should be drawn before the intended sample size is reached. Concerning the absolute values of the parameters, a systematic underestimation of the CBF compared to the literature8-9 was observed. This might be due to partial volume effects and imperfect labeling in the pCASL sequence. The OEF was systematically overestimated compared to other studies,6,10 which could be partly caused by the underestimation of CBF and thus DBV. Since the OEF was derived from three separate sequences, this parameter is especially prone to error propagation. A significant difference was found for OEF, CBF and CMRO2 in the comparison of GM and WM both in pre- and post-smoking state. CBF and CMRO2 are meant to reveal GM-WM contrast; however, the OEF is usually considered to be uniform throughout the brain.10 Yet, similar contrast has been observed in other multi-parametric OEF studies.11 This study did not distinguish between age and different smoking habits of the subjects; yet, this could be a considerable source of parameter variation. The so far small sample size will be increased by examining 15 further smokers in the course of this study.Conclusion
In this multi-parametric quantitative BOLD study no significant difference in brain oxygenation and perfusion was found in 5 chronic smokers before and after acute nicotine administration. However, further 15 participants will be included in this study before final conclusions can be drawn.Acknowledgements
*Both authors contributed equally to this work.References
1. Rose JE, Behm FM, Westman EC, Mathew RJ, London ED, Hawk TC, et al. PET studies of the influences of nicotine on neural systems in cigarette smokers. Am J Psychiatry. 2003;160:323–333.
2. Yamamoto Y, Nishiyama Y, Monden T, Satoh K, Ohkawa M. A study of the acute effect of smoking on cerebral blood flow using 99mTc-ECD SPET. Eur J Nucl Med Mol Imaging. 2003;30:612–614.
3. Song Y, Kim Jg, Cho HJ, Kim JK, Suh DC. Evaluation of cerebral blood flow change after cigarette smoking using quantitative MRA. PLOS ONE. 2017;12(9):e0184551
4. Alsop DC, Detre JA, Golay X, et al. Recommended implementation of arterial spin-labeled Perfusion MRI for clinical applications: A consensus of the ISMRM Perfusion Study group and the European consortium for ASL in dementia. Magn Reson Med 2015;73(1):102-116.
5. Ciris, P. A., Qiu, M. and Constable, R. T. (2014), Noninvasive MRI measurement of the absolute cerebral blood volume–cerebral blood flow relationship during visual stimulation in healthy humans. Magn. Reson. Med., 72: 864-875
6. An H, Lin W. Cerebral venous and arterial blood volumes can be estimated separately in humans using magnetic resonance imaging. Magn Reson Med 2002;48(4):583-588.
7. Skinhoj E, Olesen J, Paulson OB. Influence of smoking and nicotine on cerebral blood flow and metabolic rate of oxygen in man. J Appl Physiol. 1973;35(6):820–2.
8. Christen T, Schmiedeskamp H, Straka M, Bammer R, Zaharchuk G. Measuring brain oxygenation in humans using a multiparametric quantitative blood oxygenation level dependent MRI approach. Magn Reson Med. 2012;68(3):905–11.
9. Ito H, Kanno I, Kato C, Sasaki T, Ishii K, Ouchi Y, et al. Database of normal human cerebral blood flow, cerebral blood volume, cerebral oxygen extraction fraction and cerebral metabolic rate of oxygen measured by positron emission tomography with 15O-labelled carbon dioxide or water, carbon monoxide and oxygen. Eur J Nucl Med Mol Imaging. 2004;31(5):635–43.
10. Raichle ME, Macleod AM, Snyder AZ, Powers WJ, Gusnard DA, Shulman GL. A default mode of brain function. Proc Natl Acad Sci USA. 2001;98(2):676–82.
11. Hirsch NM, Toth V, Förschler A, Kooijman H, Zimmer C, Preibisch C. Technical considerations on the validity of blood oxygenation level‐dependent‐based MR assessment of vascular deoxygenation. NMR Biomed. 2014;27:853-862.
Figures