2923
A Dedicated Framework for Intracranial Vessel Wall Imaging: Optimized 3D Dark-blood Imaging and Automated Post-processing1Diagnostic and Interventional Radiology, University Hospital Würzburg, Würzburg, Germany, 2Radiology, Medical Physics, Medical Center – University of Freiburg, Faculty of Medicine, University of Freiburg, Freiburg, Germany, 3Siemens Healthineers, Erlangen, Germany, 4Neuroradiology, Medical Center – University of Freiburg, Faculty of Medicine, University of Freiburg, Freiburg, Freiburg, Germany
Synopsis
MRI has been demonstrated as an indispensable imaging modality in the context of vasculitis – an inflammation of the arterial vessel wall. However, the extent of involvement of intracranial vessels is still part of on-going research. Depiction of intracranial vessels could be achieved with intracranial vessel wall imaging (VWI), which is, however, challenging because of the need for high-resolution within acceptable scan times. Further, the visual assessment of intracranial mural changes is also difficult because of the tortuous vessel course. Our work describes a framework for intracranial VWI with an optimized, compressed-sensing-accelerated sequence prototype and dedicated VWI post-processing.
Introduction
Vasculitis is a mural inflammation of blood vessels affecting arteries of nearly any size. MRI has become one of the most important imaging modalities in the management of such patients. For example, MRI has been demonstrated an accurate tool in the initial diagnosis of giant cell arteritis1. However, the potential extent of involvement of intracranial vessels in cerebral vasculitis is still part of on-going research2 and remains to be resolved.
However, intracranial vessel wall imaging (VWI) is still challenging because of the need for isotropic, high spatial resolution (<< 1mm) and whole brain coverage within clinically acceptable scan times, especially when pre- and post-contrast images are acquired for unambiguous assessment of inflammatory changes. The visual assessment of intracranial mural changes is also difficult because of the tortuous vessel course. Here, a visualization plane would be favorable which is oriented according to the local vessel track. This, however, cannot be achieved with a single plane orientation.
Our work describes a framework for intracranial VWI with an optimized, compressed-sensing (CS)-accelerated, high-resolution 3D sequence in combination with an automated post-processing tool for evaluation of pre- and post-contrast images in arbitrary plane orientations.
Methods
3D Intracranial VWI
The tortuous course of intracranial vessels makes 3D imaging preferable because isotropic 3D data can be reformatted in arbitrary orientations3. High-resolution whole-brain intracranial VWI can be done with variable-flip-angle 3D turbo spin echo sequences (such as Sampling Perfection with Application optimized Contrasts using different flip angle Evolution – SPACE) providing an intrinsic dark-blood effect. However, such sequences still require scan times of about 10 min even when using parallel imaging and/or partial Fourier4,5.
Recently, a CS-accelerated SPACE sequence prototype was introduced revealing its potential for assessment of cerebral vascular diseases6. The sequence uses pseudo-random Poisson-disc variable-density k-space sampling7 with elliptical coverage to ensure incoherent undersampling artifacts. Reconstruction is done via an iterative (here: Niter = 20) sensitivity encoding-type reconstruction combined with L1-norm-based regularization6-8. Based on the prior study6, we implemented a sagittal whole-brain T1-weighted CS-SPACE protocol on a 3T whole-body scanner (MAGNETOM Prisma, Siemens Healthineers, Erlangen, Germany) to provide an isotropic resolution of 0.55 mm within a scan time of 5:50 min. The final protocol comprised an echo train length of 50 to compromise between blurring and time-efficient sampling. The k-space undersampling factor was set to 0.22 yielding an approximate 5-fold acceleration compared to full k-space sampling. Imaging was done with the system’s 64-channel head coil (further scan parameters: TR/TE = 800/10 ms, FOV = 210×210×140 mm3, matrix = 384×384×256, pixel bandwidth = 450 Hz/px).
Post-processing Algorithm
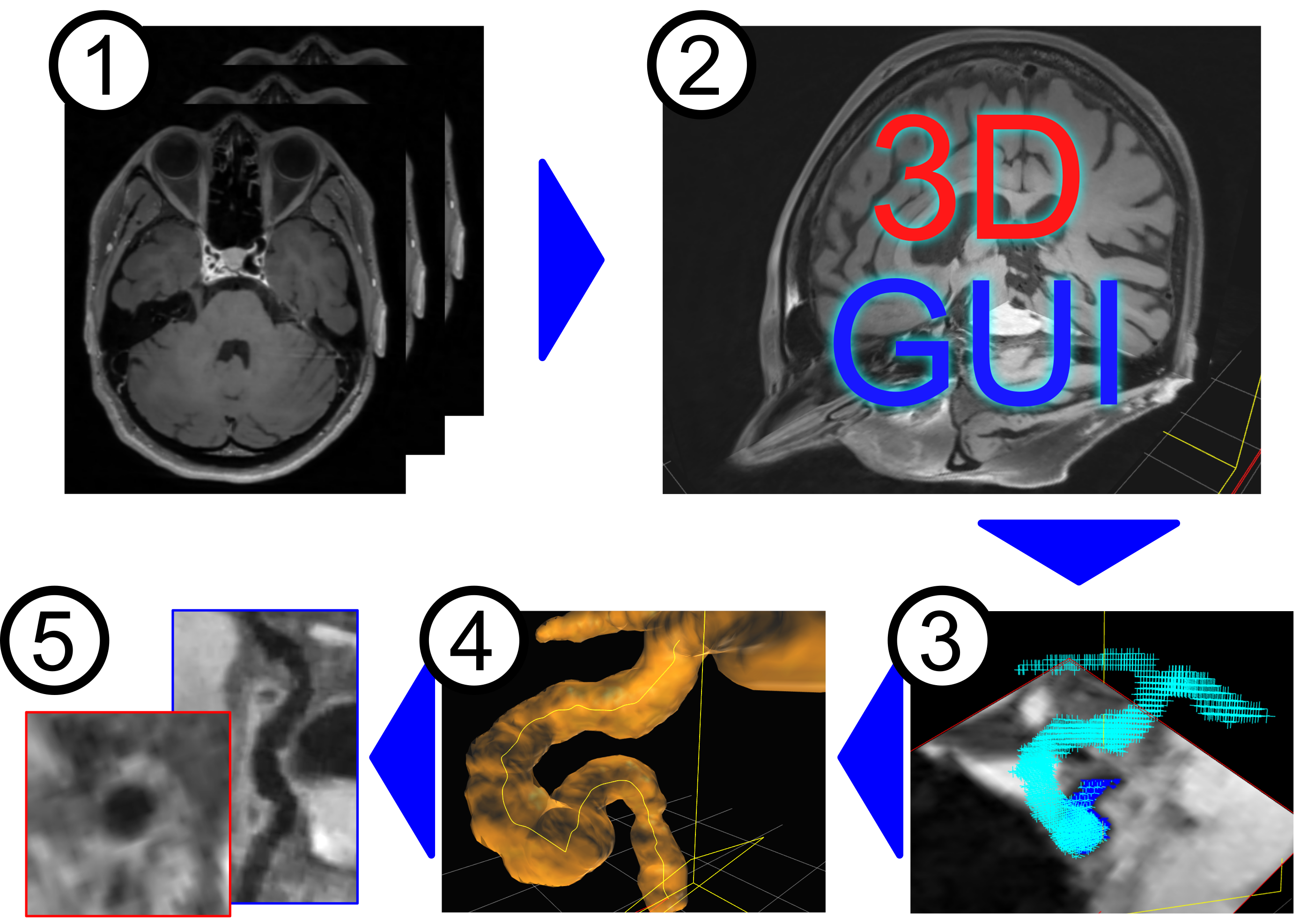
The assessment of tortuous intracranial vessels requires a robust technique for 3D extraction of the curved tubular vascular structure which could in general be achieved via a range of approaches9. The workflow of our post-processing approach is summarized in Fig. 1. The algorithm is designed to directly extract vascular structures from the 3D dark-blood data (step 1). Initially, multiple seed-points have to be defined in the vessel of interest via an easy-to-use graphical user interface (step 2). They serve as starting points for an iterative voxel-based inflation via a modified Dijkstra algorithm10 to segment the vessel volume (step 3). Then, the centerline is automatically detected11 to trace the central voxel path through the vessel (step 4). Smoothing of the centerline is achieved with a 3D Bézier interpolation algorithm, and a 3D-mesh model is extracted by a marching-cube algorithm used for 3D visualization of the vessel structure (also illustrated in step 4). Finally, the centerline’s trajectory is used to reconstruct reformatted views12 of the tortuous vessel structure in planar (curved planar reformation – CPR) and perpendicular orientations (step 5) to provide optimized visualization planes for assessment of the vessel wall.
Results and Discussion
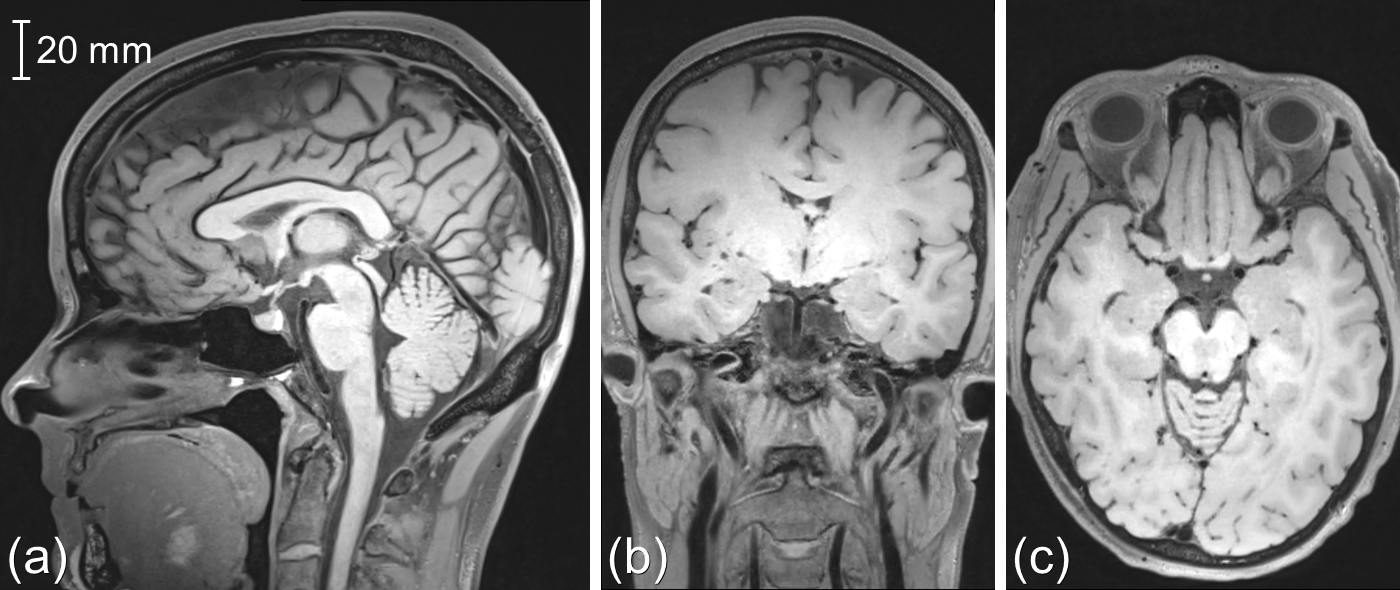
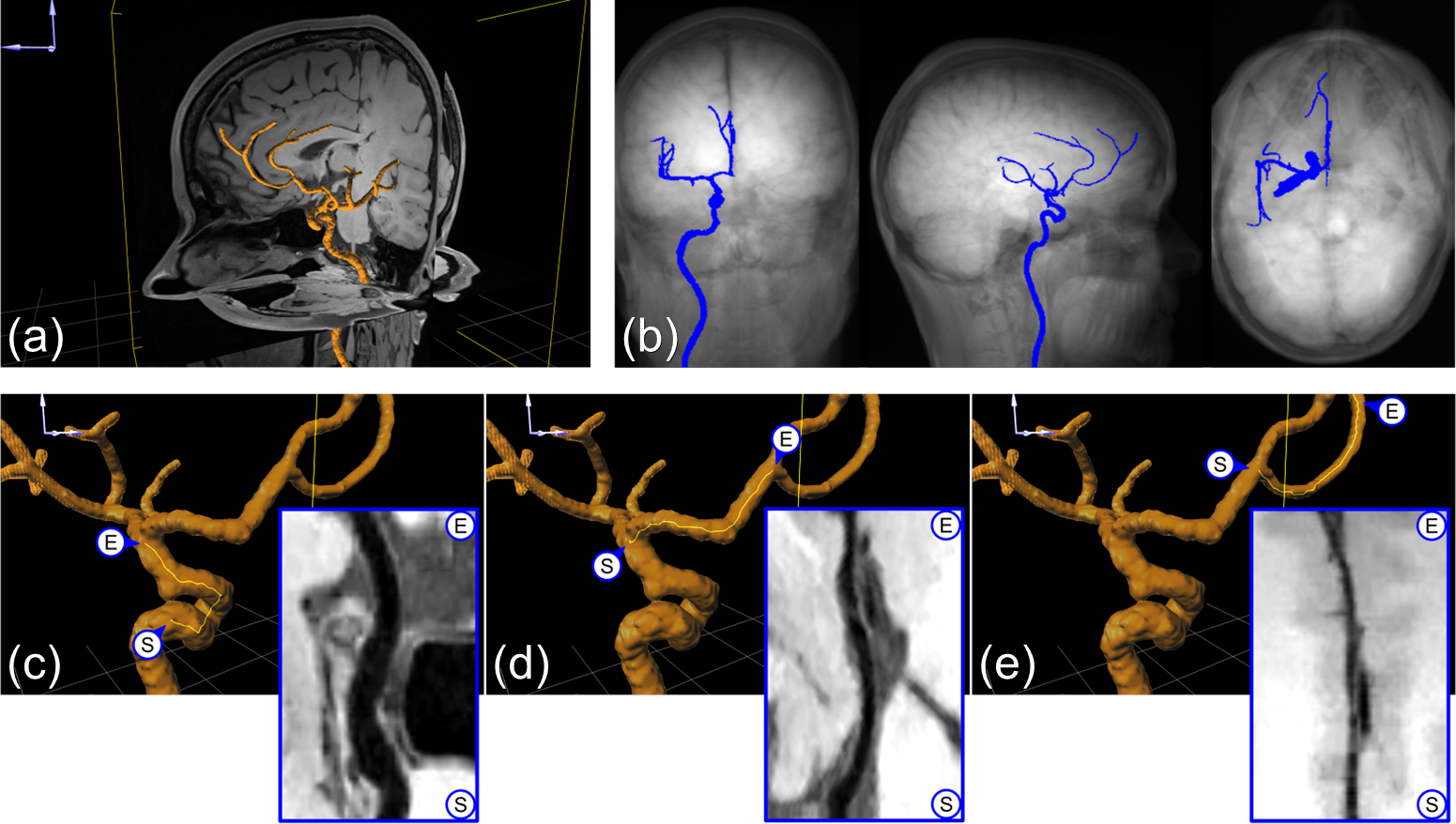
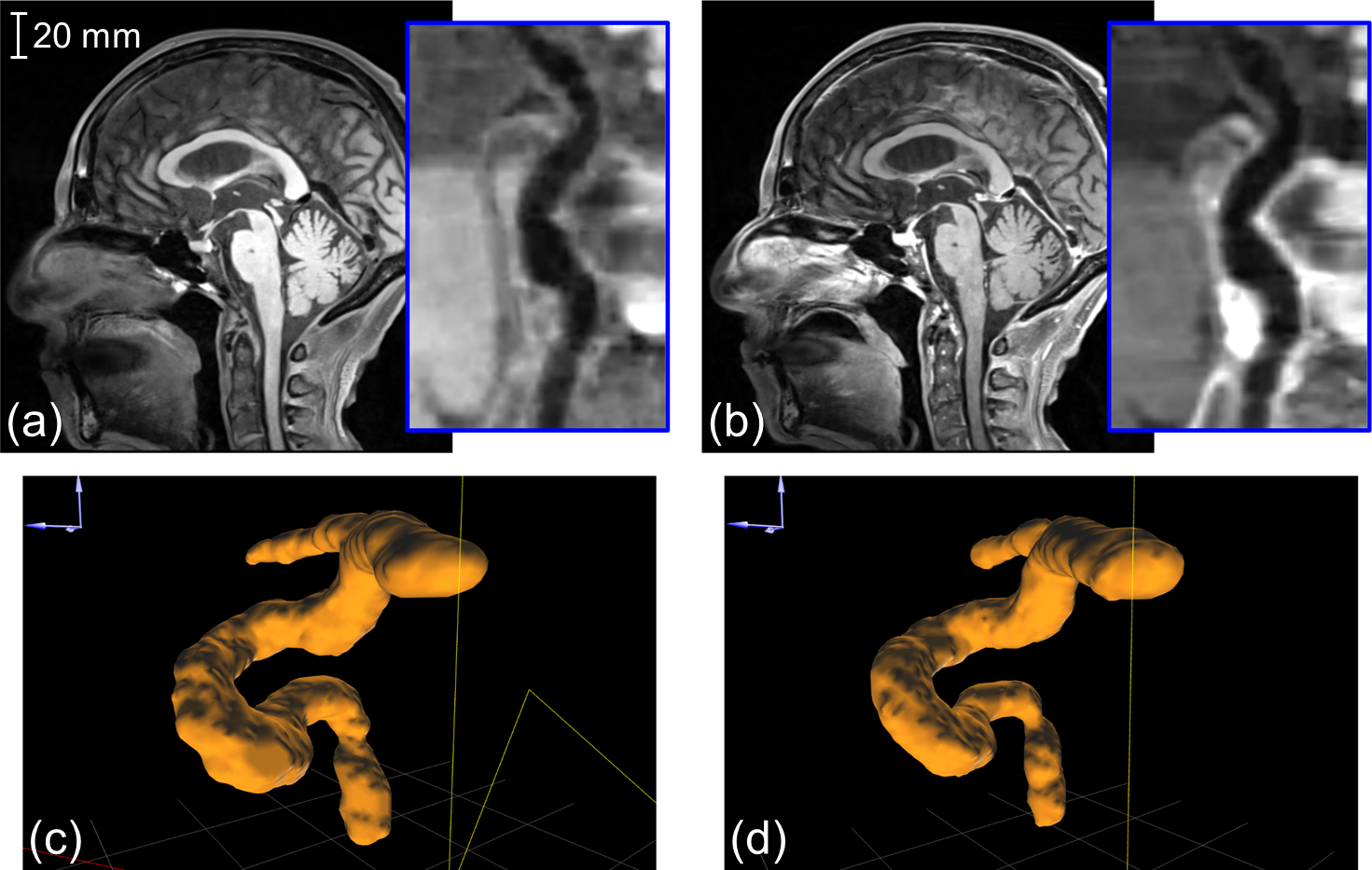
Figure 2 illustrates representative images acquired with the optimized CS-SPACE protocol in a healthy volunteer. In Fig. 3, centerline and 3D mesh of the automatically segmented arteries (internal carotid artery (ICA), middle and anterior cerebral artery) are shown. For technical proof-of-concept in a clinical situation, pre- and post-contrast CPR views of the ICA in a patient with confirmed giant cell arteritis are presented in Fig. 4. Without further training, CPR reformats could be generated within less than 10 min.
Our pilot findings demonstrate the successful reconstruction of CPR reformats from high-resolution 3D dark-blood CS-SPACE data for assessment of mural inflammatory changes of intracranial arteries. Our approach enables optimized visualization of the tortuous intracranial arteries and readily reveals mural thickness and contrast enhancement in any vessel segment. Further studies are warranted for evaluation of its clinical use.
Acknowledgements
Grant support by the Deutsche Forschungsgemeinschaft (DFG) under grant numbers DFG HE 1875/26-2, and BL1132/1-2 is greatly acknowledged.References
[1] Klink T, Geiger J, Both M, Ness T, Heinzelmann S, Reinhard M, Holl-Ulrich K, Duwendag D, Vaith P, Bley TA. Giant cell arteritis: diagnostic accuracy of MR imaging of superficial cranial arteries in initial diagnosis-results from a multicenter trial. Radiology. 2014 Dec;273(3):844-52.
[2] Siemonsen S, Brekenfeld C, Holst B, Kaufmann-Buehler AK, Fiehler J, Bley TA. 3T MRI reveals extra- and intracranial involvement in giant cell arteritis. AJNR Am J Neuroradiol. 2015 Jan;36(1):91-7.
[3] Mandell DM, Mossa-Basha M, Qiao Y, Hess CP, Hui F, Matouk C, Johnson MH, Daemen MJ, Vossough A, Edjlali M, Saloner D, Ansari SA, Wasserman BA, Mikulis DJ. Intracranial Vessel Wall MRI: Principles and Expert Consensus Recommendations of the American Society of Neuroradiology. AJNR Am J Neuroradiol. 2017 Feb;38(2):218-229.
[4] Zhu C, Haraldsson H, Tian B, Meisel K, Ko N, Lawton M, Grinstead J, Ahn S, Laub G, Hess C, Saloner D. High resolution imaging of the intracranial vessel wall at 3 and 7 T using 3D fast spin echo MRI. MAGMA. 2016 Jun;29(3):559-70.
[5] Fan Z, Yang Q, Deng Z, Li Y, Bi X, Song S, Li D. Whole-brain intracranial vessel wall imaging at 3 Tesla using cerebrospinal fluid-attenuated T1-weighted 3D turbo spin echo. Magn Reson Med. 2017 Mar;77(3):1142-1150.
[6] Zhu C, Tian B, Chen L, Eisenmenger L, Raithel E, Forman C, Ahn S, Laub G, Liu Q, Lu J, Liu J, Hess C, Saloner D. Accelerated whole brain intracranial vessel wall imaging using black blood fast spin echo with compressed sensing (CS-SPACE). MAGMA. 2018 Jun;31(3):457-467.
[7] Li G, Zaitsev M, Büchert M, Raithel E, Paul D, Korvink JG, Hennig J. Improving the robustness of 3D turbo spin echo imaging to involuntary motion. MAGMA. 2014 Aug;28:329–345.
[8] Fritz J, Raithel E, Thawait GK, Gilson W, Papp DF. Six-Fold Acceleration of High-Spatial Resolution 3D SPACE MRI of the Knee Through Incoherent k-Space Undersampling and Iterative Reconstruction-First Experience. Invest Radiol. 2016 Jun;51(6):400-9.
[9] C. Kirbas and F. Quek, A Review of Vessel Extraction Techniques and Algorithms. ACM Computing Surveys. 2004 Jun;36(2):81–121.
[10] E.W. Dijkstra, A note on two problems in connexion with graphs, Numerische Mathematik. 1959;1:269-71.
[11] ChengY, Hu X, Wang Y, Wang J, Tamura S. Automatic centerline detection of small three-dimensional vessel structures, J Electron Imag. 2014;23(1):013007.
[12] Williams D, Grimm S, Coto E, Roudsari A, Hatzakis H. Volumetric Curved Planar Reformation for Virtual Endoscopy, IEEE Trans Vis Comput Graph. 2007;14(1):109-19.
Figures