2922
Reduced Cerebral Blood Flow in Aging Adults with Down Syndrome: An Arterial Spin Labeling Study1F. Joseph Halcomb III, MD Department of Biomedical Engineering, University of Kentucky, Lexington, KY, United States, 2MD/PhD Program, University of Kentucky, Lexington, KY, United States, 3Pharmacology & Nutritional Sciences, University of Kentucky, Lexington, KY, United States, 4Sanders-Brown Center on Aging, University of Kentucky, Lexington, KY, United States, 5Molecular & Cellular Biochemistry, University of Kentucky, Lexington, KY, United States, 6Pharmaceutical Sciences, University of Kentucky, Lexington, KY, United States, 7Health Sciences - Rehabilitation Science, University of Kentucky, Lexington, KY, United States, 8MAgnetic Resonance Imaging and Spectroscopy Center, University of Kentucky, Lexington, KY, United States, 9Neuroscience, University of Kentucky, Lexington, KY, United States, 10Neurology, University of Kentucky, Lexington, KY, United States, 11Behavioral Science, University of Kentucky, Lexington, KY, United States, 12Pediatric Neurology, University of Kentucky, Lexington, KY, United States, 13Magnetic Resonance Imaging and Spectroscopy Center, University of Kentucky, Lexington, KY, United States, 14Psychiatry, University of Kentucky, Lexington, KY, United States
Synopsis
Adults with Down syndrome (DS) represent an important model of Alzheimer disease in the absence of cerebrovascular disease (CVD) risk factors like atheroma and hypertension. In this study we used pulsed arterial spin labeling (PASL) to measure cerebral blood flow (CBF) in aging adults with DS and age-matched controls. In adults with DS there is a 31% reduction in CBF after the age of 54 (<54= 46.7mL/100g/min, >54= 32.3mL/100g/min, p=0.011). Despite their CVD protective phenotype, adults with DS do develop vascular dysfunction, however the onset is concurrent with dementia rather than preceding it.
Introduction
People with trisomy 21, or Down syndrome (DS), are at high risk for developing dementia due to the overexpression of amyloid precursor protein on chromosome 211. This population typically develops observable Alzheimer disease (AD) neuropathology after 30 years of age2, but they also exhibit a number of protective cardiovascular traits such as the absence of atheroma and hypertension3,4. With an increasing recognition of cerebrovascular disease (CVD) as a critical comorbidity for AD5,6, the DS population represents a unique cohort to study AD progression in the absence of confounding CVD. In this study we used arterial spin labeling (ASL) to measure cerebral blood flow (CBF) in a group of DS participants as well as age-matched controls to test the hypothesis that CBF will be compromised in people with DS despite protective vascular risk factors.Methods
Adults with DS were recruited through local DS support groups and residential facilities as a part of an ongoing longitudinal study of aging in DS (n=35, aged 26-65yrs). Fifteen age-matched controls were also recruited.
Imaging Protocol: We used a pulsed ASL (PASL) sequence with a 3-D gradient and spin echo (GRASE) readout for CBF measurement7. Parameters: TR/TE/TI (inflow time)/TS (saturation time) = 4500/13.04/1900/1400ms, slab thickness =154mm, slice-selective labeling gradient =10mT/m, matrix = 64x64x44, FOV = 224x224x154mm. Data sets were then coregistered using an intensity-based registration algorithm in Matlab (Mathworks, Natick, MA, USA) before being averaged to yield a control, a labeled and an M0 volume for each subject. Quantitative CBF maps (in ml/100g/min) were calculated using in-house Matlab software applying the equation8
$$CBF(mL/100g/min)=\frac{6000\times\lambda\times e^{\left(\frac{PLD}{T_{1,Blood}}\right)}}{2\times\alpha\times\left(1-e^{\left(\frac{LD}{T_{1,Blood}}\right)}\right)}\times\frac{Ctl-Lbl}{M_0} $$
where λ is the blood-brain partition coefficient (assumed to be 0.9 mL/g), Ctl and Lbl are the average signal intensity of the control and labeled volumes respectively, T1,blood is the longitudinal relaxation time of the blood (assumed to be 1.65 seconds at 3.0T), M0 is the average signal intensity of the M0 volumes, and α is the labeling efficiency (assumed to be 0.98 for PASL) .
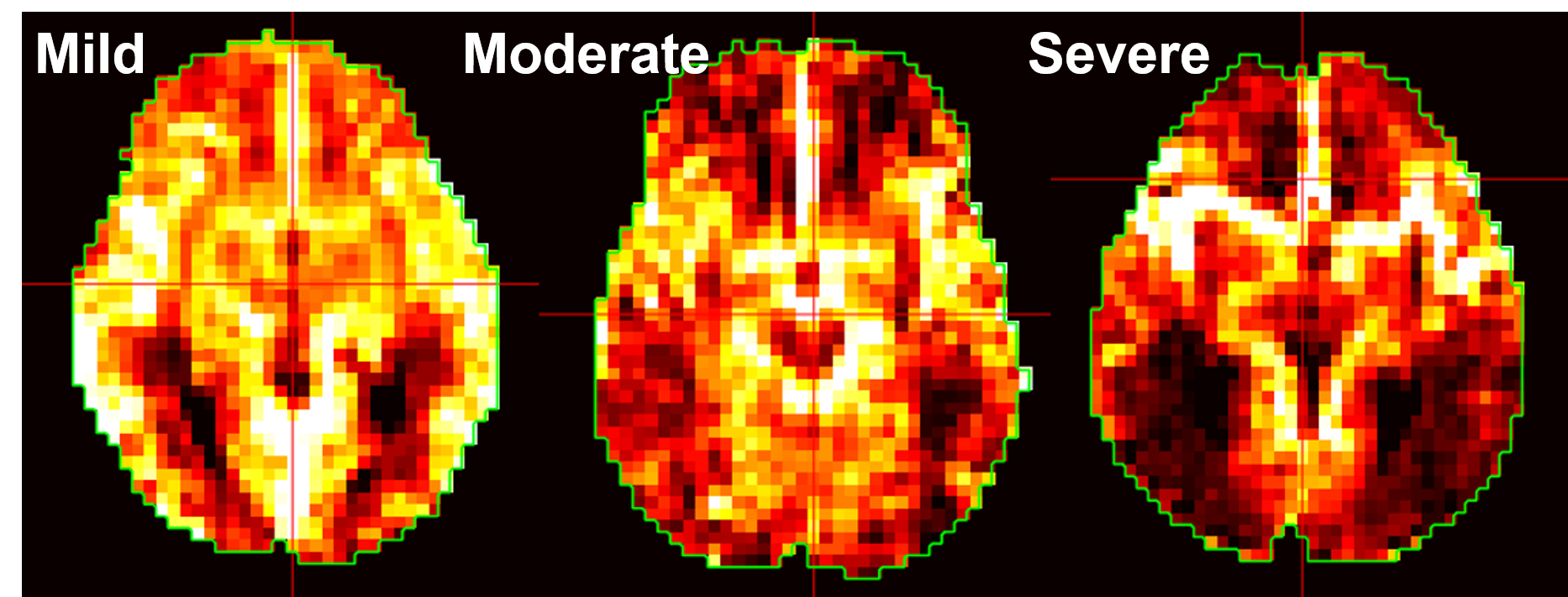
Image Analysis: A single ROI encompassing the entire brain volume was drawn manually with the assistance of the in-house Matlab software. Global CBF was calculated as the average of all voxels in the ROI. In some subjects a large portion of the ASL signal was retained in the large arteries of the brain, so to quantify the effect of this residual arterial signal (RAS), the same axial slice from each subject received a rating of minimal, moderate, or severe RAS. An example for each rating is shown in Figure 1.
Results
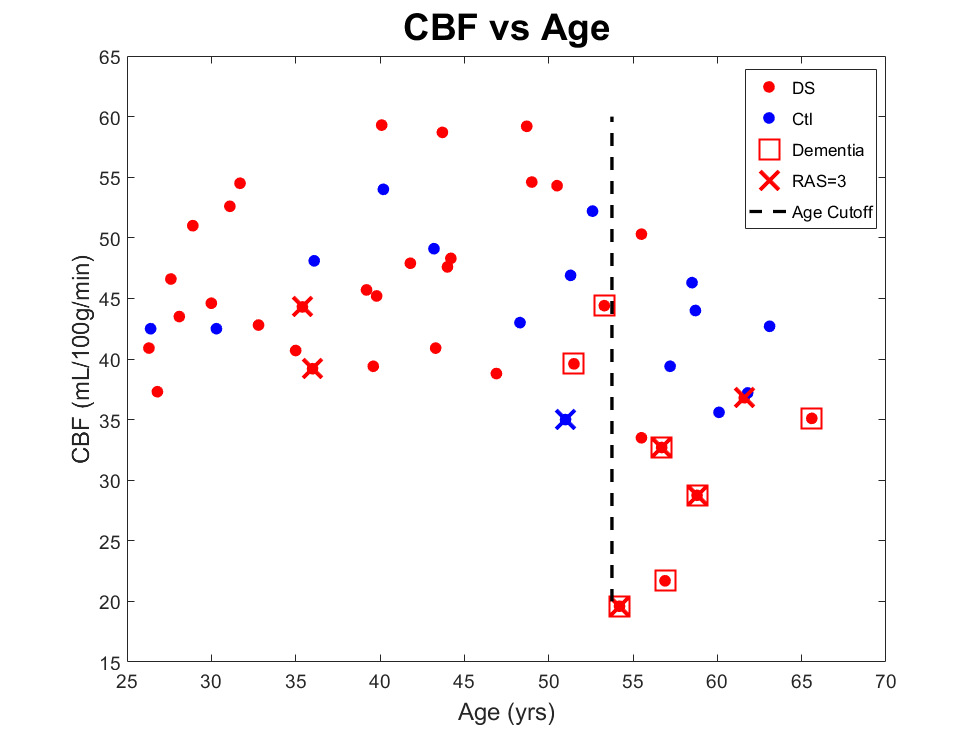
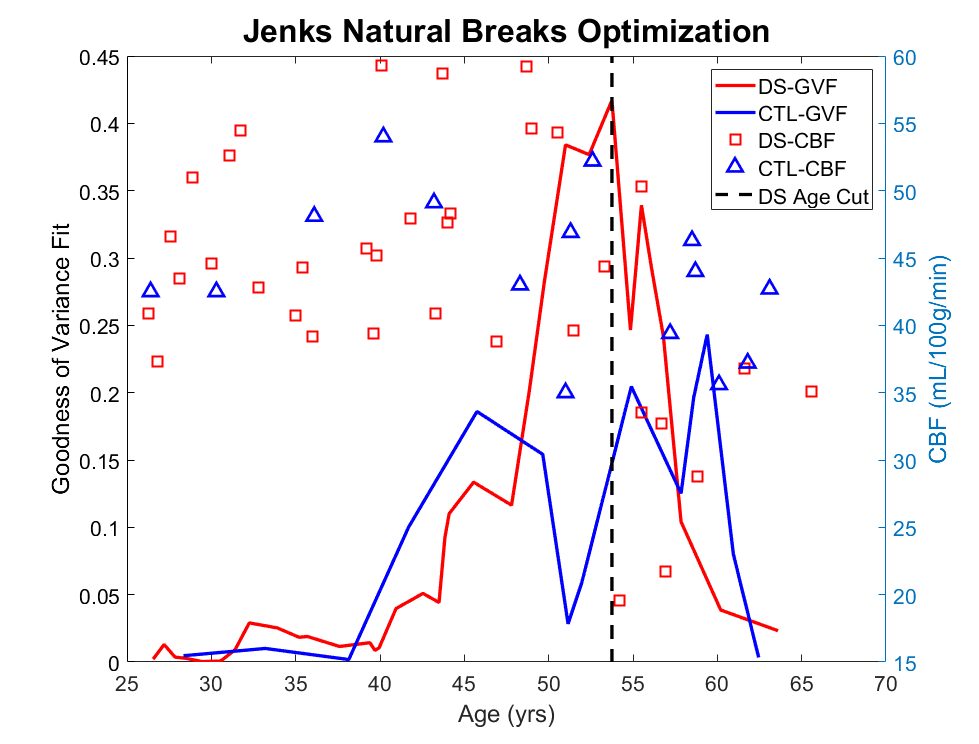
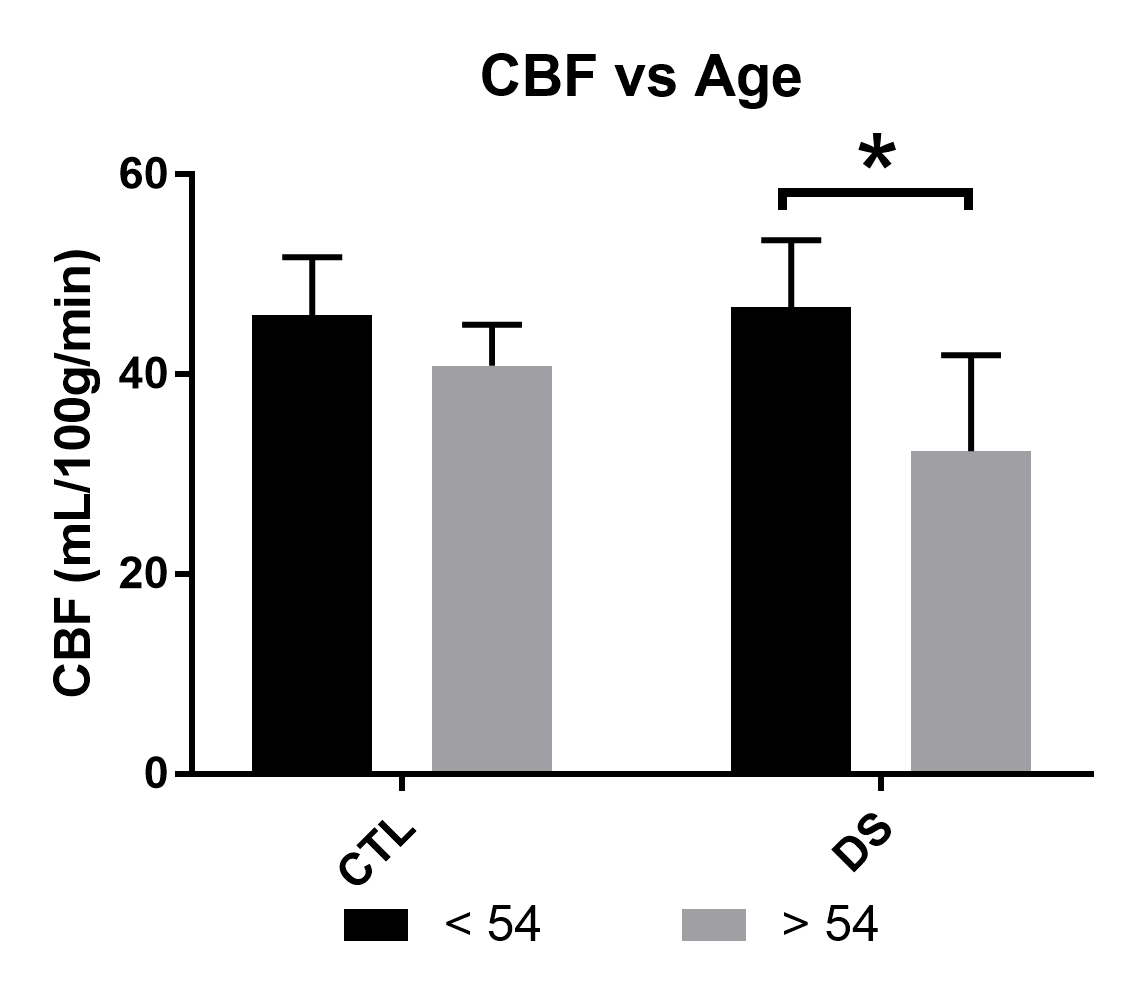
A plot of global CBF versus age reveals a clustering of DS participants over the age of 54 with drastically reduced CBF values (see Figure 2). This clustering is confirmed by Jenks natural breaks optimization9 which showed a maximal goodness of variance fit at age 53.75 (see Figure 3). DS participants older than the cut-off age of 54 had a 31% reduction in CBF (32.3± 9.6mL/100g/min) versus younger people with DS (46.7± 6.7mL/100g/min, p=0.011) (See Figure 4). This comparison was significant when controlling for RAS score and sex. No such pattern is observed in the control group (young= 45.9± 5.8mL/100g/min, old= 40.9± 4.1mL/100g/min). The same cluster of people with DS over the age of 54 also had a significantly higher proportion of severe RAS scores (50%) vs younger people with DS (7%, p=0.005) or non-DS controls (7%, p=0.016), and prevalence of diagnosed dementia (older DS=60%, younger DS=7% p<0.001, Ctl =0% p<0.001).Discussion
In adults with DS there is a drastic reduction in global CBF after the age of 54. That this compromise in perfusion occurs in the 6th decade with the transition to dementia rather than in the 5th decade during the rapid accumulation of amyloid plaque suggests that the CVD protective phenotype of DS works to preserve perfusion, but this mechanisms is ultimately overwhelmed resulting in vascular deficits that can be observed using PASL. This is supported by evidence in the literature of abundant cerebral amyloid angiopathy in older individuals with DS10,11. However, this pattern of reduced CBF differs from the progression of hypoperfusion in late-onset AD, which typically precedes dementia by decades12.Conclusion
This study has demonstrated that adults with DS exhibit deficits in perfusion that do not occur until the transition to dementia as opposed to other forms of AD where perfusion deficits precede dementia. This suggests a relationship between AD progression and concomitant CVD that could be amenable to intervention aimed at reducing the risk for vascular dysfunction.Acknowledgements
R01HD064993 from NIH/NICHD
T32 AG057461
References
1. Doran E, Keator D, Head E, et al. Down Syndrome, Partial Trisomy 21, and Absence of Alzheimer's Disease: The Role of APP. J Alzheimers Dis. 2017;56(2):459-470.
2. Head E, Lott IT, Wilcock DM, Lemere CA. Aging in Down Syndrome and the Development of Alzheimer's Disease Neuropathology. Curr Alzheimer Res. 2016;13(1):18-29.
3. Brattstrom L, Englund, E., Brun, A. Does Down syndrome support homocysteine theory of arteriosclerosis. Lancet. 1987;14(8529):391-392.
4. Murdoch JC, Rodger, J.C., Rao, S.S., Fletcher, C.D., Dunningham, M.G. Down's syndrome: an atheroma-free model? . Br Med J. 1977;2(6081):226-228.
5. Kapasi A, Schneider JA. Vascular contributions to cognitive impairment, clinical Alzheimer's disease, and dementia in older persons. Biochim Biophys Acta. 2016;1862(5):878-886.
6. Snyder HM, Corriveau RA, Craft S, et al. Vascular contributions to cognitive impairment and dementia including Alzheimer's disease. Alzheimers Dement. 2015;11(6):710-717.
7. Fernández‐Seara MA, Wang Z, Wang J, et al. Continuous arterial spin labeling perfusion measurements using single shot 3D GRASE at 3 T. Magnetic Resonance in Medicine. 2005;54(5):1241-1247.
8. Alsop DC, Detre JA, Golay X, et al. Recommended implementation of arterial spin-labeled perfusion MRI for clinical applications: A consensus of the ISMRM perfusion study group and the European consortium for ASL in dementia. Magn Reson Med. 2015;73(1):102-116.
9. Jenks GF. The Data Model Concept in Statistical Mapping. International Yearbook of Cartography. 1967;7:186-190.
10. Wilcock DM, Schmitt FA, Head E. Cerebrovascular contributions to aging and Alzheimer's disease in Down syndrome. Biochim Biophys Acta. 2016;1862(5):909-914.
11. Head E, Phelan MJ, Doran E, et al. Cerebrovascular pathology in Down syndrome and Alzheimer disease. Acta Neuropathol Commun. 2017;5(1):93.
12. Iturria-Medina Y, Sotero RC, Toussaint PJ, Mateos-Perez JM, Evans AC. Early role of vascular dysregulation on late-onset Alzheimer's disease based on multifactorial data-driven analysis. Nat Commun. 2016;7:11934.
Figures