2919
Amide proton transfer (APT) MRI is a predictor of survival and progression in high-grade glioma patients1Radiology, German Cancer Research Center, Heidelberg, Germany, 2Medical Physics in Radiology, German Cancer Research Center, Heidelberg, Germany, 3Radiology, University Hospital Essen, Essen, Germany, 4Max-Planck-Institut Tuebingen, Tuebingen, Germany, 5Neurosurgery, University of Heidelberg, Heidelberg, Germany, 6Neurology, University of Heidelberg, Heidelberg, Germany, 7Neuroradiology, University of Heidelberg, Heidelberg, Germany
Synopsis
In this work we show that relaxation-compensated amide proton transfer (APT) imaging at 7.0 T is associated with overall survival and progression-free survival in newly-diagnosed, previously untreated glioma patients. The current study showed that glioma patients with increased APT values were more likely to progress sooner and live shorter, respectively. This effect may be caused by strong alterations of amino acid concentrations and global upregulation of protein expression in more aggressive brain tumors. Therefore, APT CEST imaging may help to enhance the prognostic value of non-invasive MRI tools at the time of initial diagnosis and during follow-up.
Background and Purpose
Methods
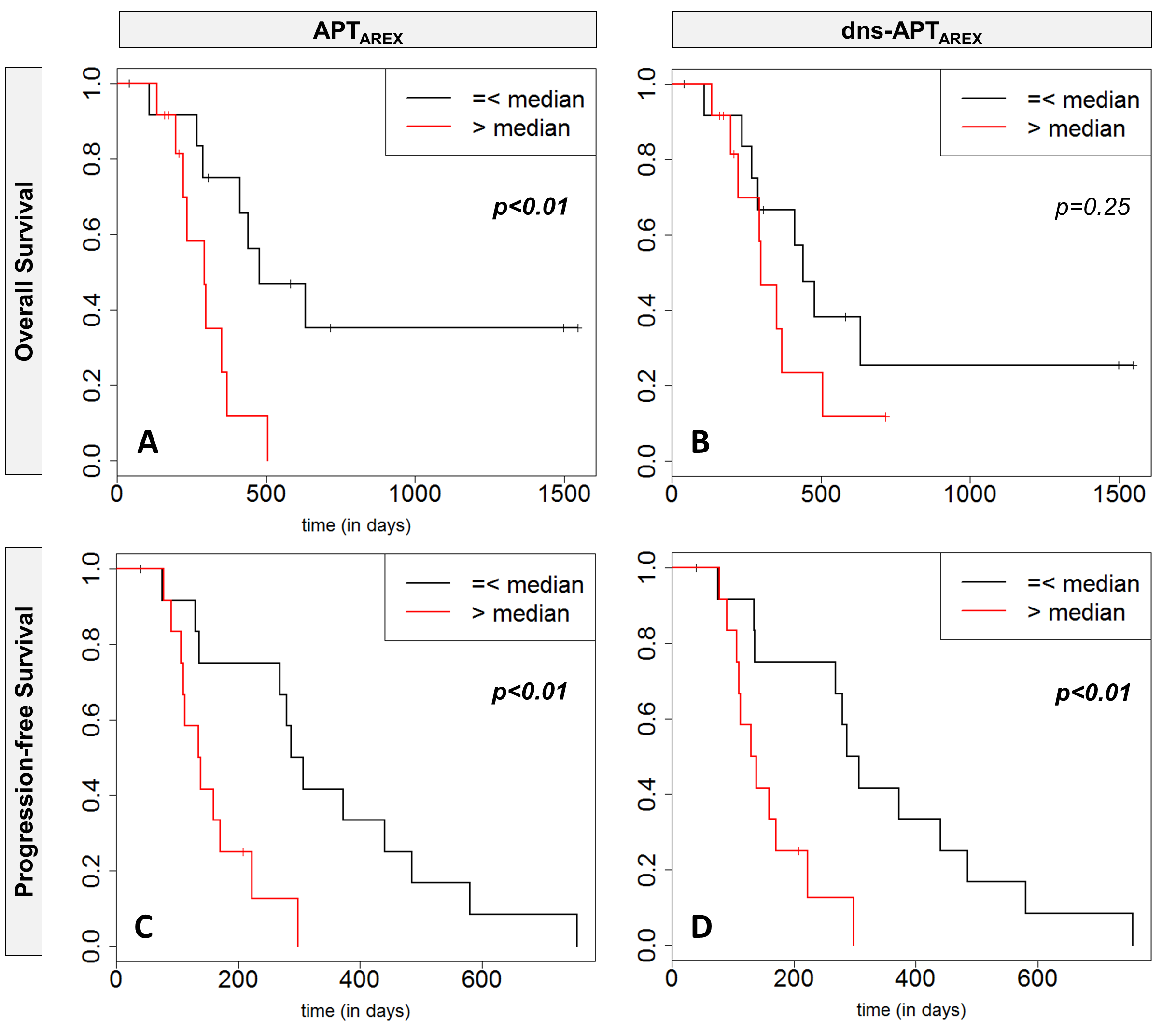
Twenty-six patients with newly-diagnosed high-grade glioma (WHO grade III-IV) were included in this prospective IRB-approved study. CEST MRI was performed on a 7.0 Tesla whole-body scanner. APT-weighted CEST contrasts were calculated using the relaxation-compensated apparent exchange-dependent relaxation (AREX) approach [2] and the downfield relayed nuclear Overhauser effect (rNOE)-suppressed APT (dns-APTAREX) metric [3]. B0 and B1 field inhomogeneities were determined using the water shift and B1 method (WASABI) [4] and reconstructed corresponding to B1=0.6 µT saturation amplitude [5]. Association of patient OS and PFS with relaxation-compensated APT MRI (APTAREX and dns-APTAREX) were assessed using the univariate Cox proportional-hazards regression model. Hazard ratios (HR) and corresponding 95% confidence intervals were calculated. Moreover, Kaplan-Meier analyses with two-sided log-rank statistics were additionally performed for OS and PFS for both APT contrasts after dichotomization into two groups at the median. Furthermore, OS/PFS association with clinical parameters (age, gender, O6-methylguanine-DNA methyltransferase (MGMT) promotor methylation status, and therapy: biopsy + radiochemotherapy vs. debulking surgery + radiochemotherapy) were tested accordingly.Results
The APTAREX contrast was significantly associated with patient OS (HR=3.15, p=0.02) and PFS (HR=1.83, p=0.009). Median OS/PFS of patients with low tumor signal intensities (APTAREX ≤4.23%) was 411/293 days compared to 292/112 days for patients with increased APT values (APTAREX>4.23%) (Fig. 1A,C). Strongest association with PFS was found for the dns-APT metric (HR=2.61, p=0.002) (Fig. 1D). Among the tested clinical parameters, patient age (HR=1.1, p=0.001) and therapy (HR=3.68, p=0.026) were significant for OS; age additionally for PFS (HR=1.04, p=0.048).Discussion and Conclusion
The study
showed that glioma patients with increased APT values were more likely to
progress sooner and live shorter, respectively. This effect may be caused by
strong alterations of amino acid concentrations and global upregulation of
protein expression in more aggressive brain tumors. This is
the first study reporting an association of APT MRI with overall survival and progression-free
survival in newly-diagnosed, previously untreated glioma patients. Therefore,
the study adds an important element to the fast growing body of evidence
regarding the prognostic value of CEST MRI in neuro-oncology.Acknowledgements
none.References
[1] Kim KB (2014) PFS as a surrogate for overall survival in metastatic melanoma. The Lancet Oncology 15:246-248 2
[2] Zaiss M, Windschuh J, Paech D et al (2015) Relaxation-compensated CEST-MRI of the human brain at 7 T: Unbiased insight into NOE and amide signal changes in human glioblastoma. NeuroImage 112:180-188 4
[3] Zaiss M, Windschuh J, Goerke S et al (2017) Downfield-NOE-suppressed amide-CEST-MRI at 7 Tesla provides a unique contrast in human glioblastoma. Magn Reson Med 77:196-208 5
[4] Schuenke P, Windschuh J, Roeloffs V, Ladd ME, Bachert P, Zaiss M (2017) Simultaneous mapping of water shift and B1(WASABI)—Application to field-Inhomogeneity correction of CESTMRI data. Magnetic Resonance in Medicine 77:571-580 6
[5] Windschuh J, Zaiss M, Meissner JE et al (2015) Correction of B1‐inhomogeneities for relaxation‐compensated CEST imaging at 7 T. NMR in Biomedicine 28:529-537
Figures