2899
Restriction Spectrum Imaging differentiates True Progression from Pseudoprogression in patients with high grade glioma following treatment with immunotherapyNaeim Bahrami1, Shadi Daghighi1, William Tom1, Nikdokht Farid1, and Carrie McDonald1
1University of California, San Diego, San Diego, CA, United States
Synopsis
Immunotherapy is becoming more frequently used in patients with high grade glioma (HGG) following standard chemoradiation. However, immune-mediated pseudoprogression (PsP) is a growing problem that remains poorly characterized and renders conventional imaging less useful. We evaluate the ability of a novel, advanced diffusion model, restriction spectrum imaging (RSI) to differentiate PsP from TP following immunotherapy. We demonstrate that an RSI-derived measure of axonal integrity (neurite density; ND) can differentiate TP from PsP, correctly classifying 73% of patients. We conclude that lower RSI-ND reflects disruption of axonal microstructure and may provide an imaging marker of tumor infiltration in patients with TP.
Introduction
Immunotherapy is becoming more frequently used in patients with high grade glioma (HGG) following treatment with standard chemoradiation. However, there is a growing appreciation that the local immune-mediated response may complicate the evaluation of treatment response on imaging by increasing inflammation. This inflammation can lead to the enlargement of pre-existing enhancing lesions, edema, and/or to the appearance of new enhancing lesions on MRI, mimicking true tumor progression. In this study, we evaluate whether an advanced diffusion imaging model, restriction spectrum imaging (RSI), can differentiate true progression (TP) from PsP in patients with HGG following immunotherapy. RSI uses multi-shell diffusion weightings (b-values) to separate different components of the diffusion signal, distinguishing the spherically-restricted (within cells) and cylindrically-restricted (within axons) signal from the hindered diffusion that is influenced by edema and inflammation in the extracellular matrix. In this study, we derive two measures from RSI: i.e., “RSI cellularity” (RSI-CELL) and “RSI neurite density” (RSI-ND), which provide surrogate measures of tumor cellularity and peritumoral tissue integrity, respectively. We evaluate whether RSI-CELL and RSI-ND provide better differentiation of TP from PsP compared to standard diffusion-weighted imaging (DWI) and conventional imaging.Methods
RSI, DWI, and conventional imaging was available for 19 patients with HGG who were treated with immunotherapy. Fifteen patients received an immunotherapeutic vaccine, while 4 patients received an immune checkpoint inhibitor (i.e. nivolumab) (see table1). Cases were classified as TP if pathology demonstrated recurrent tumor or if death occurred within one year of the MRI demonstrating imaging progression. The remainder of the cases were classified as PsP. Volumes of interest (VOIs) were drawn for regions of contrast enhancement (CE) and fluid attenuated inversion recovery hyperintensity (FLAIR-HI) on the first post-immunotherapy scan demonstrating imaging progression. Histogram values within VOIs were calculated for RSI-CELL, RSI-ND, and apparent diffusion coefficient (ADC) (see figure 1). Mann-Whitney U tests were used to compare RSI, ADC, and conventional imaging metrics between patients with TP versus PsP. A linear classifier with cross validation was then used to determine the combination of imaging values that best classified patients at the individual subject level. A receiver operating characteristic (ROC) curve was created to further evaluate model classification.Results
Thirteen patients showed TP and six showed PsP (Table 1). Of the six PsP cases, five were treated with a vaccine and one with a checkpoint inhibitor. Patients did not differ in their CE or FLAIR volumes. In addition, neither RSI-CELL nor ADC differentiated patients with TP from PsP, although there was a trend for patients with TP to show higher ADC compared to patients with PsP (p = 0.07) in the FLAIR-HI region. Rather, patients with TP showed a lower RSI-ND (minimum ND; p = .036) in the FLAIR-HI region compared to those with PsP (Table 2). RSI-ND correctly classified 73.3% of the sample (p = .042), with all 6 PsP cases correctly classified and 8 of 13 TP cases correctly classified. Area under curve (AUC) was 0.81 (p = .035; see figure 2).Discussion
RSI quantifies the degree to which water diffusion within tissue is driven by decreases in intra-axonal water (i.e., loss of RSI-ND) versus increases in edema/inflammation. As a result, lower RSI-ND within the FLAIR-HI region may reflect disruption of axonal microstructure, providing a robust imaging marker of tumor infiltration in patients with TP. Conversely, higher RSI-ND in the FLAIR-HI region may indicate intact axonal microstructure and a pure inflammatory response.Conclusion
We conclude that RSI measures of reduced axonal microstructure and may provide an imaging marker of tumor infiltration, differentiating TP from PsP following immunotherapy.Acknowledgements
No acknowledgement found.References
No reference found.Figures

Figure 1. Illustrates T1 post contrast, FLAIR, ADC,
RSI-ND, and RSI-CELL maps for a patient with true progression. FLAIR-HI and CE
ROIs are also overlaid on FLAIR image (bottom right)
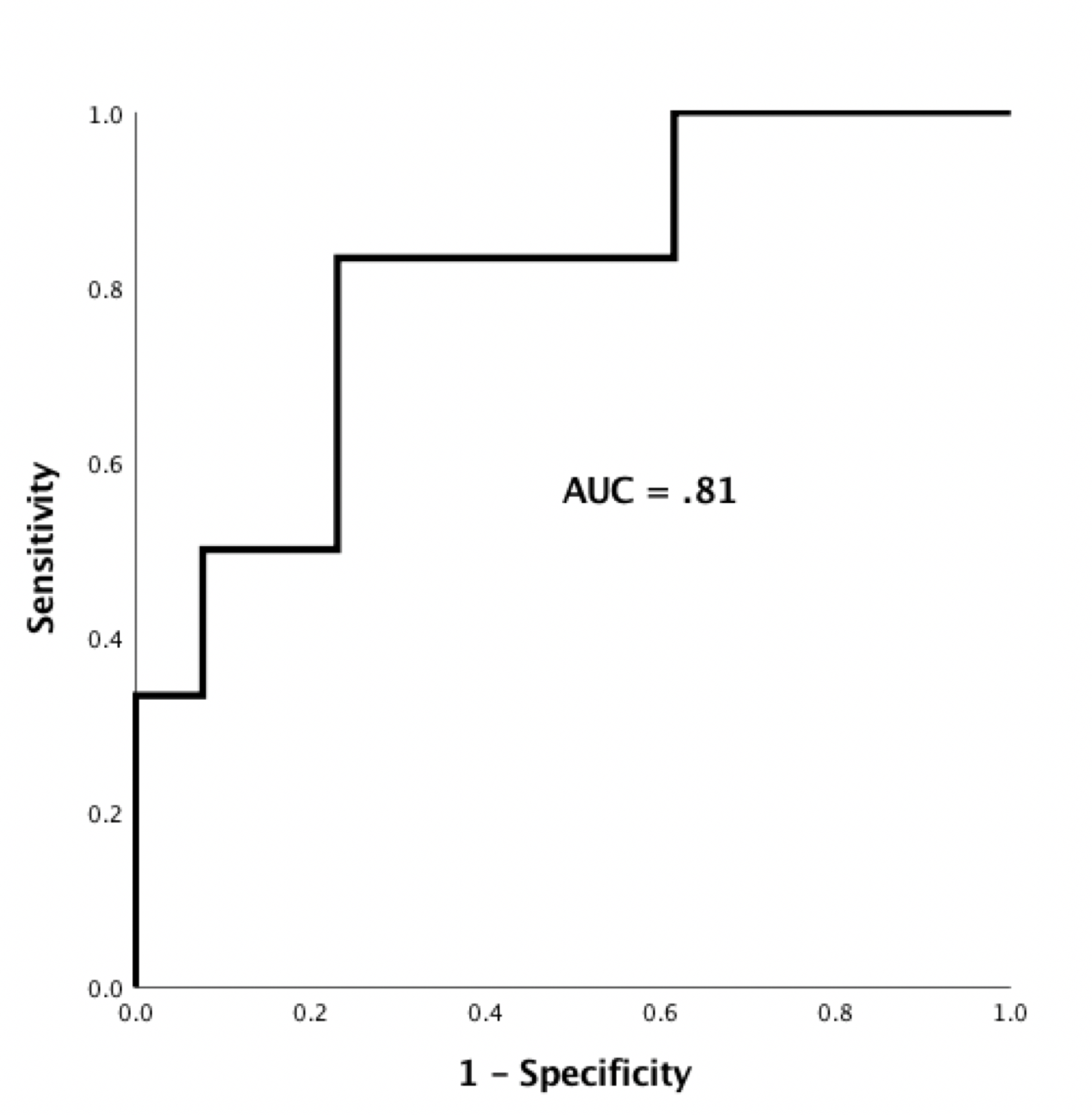
Figure 2. Illustrates the ROC curve for classifying
patients with PsP vs TP using RSI-ND marker (AUC is 0.81).

Table 1. Demonstrates patients demographic and clinical information.

Table 2. ADC and RSI parameters in the FLAIR-HI region for patients with
TP and PsP