2897
pH-weighted amine CEST-EPI as a fast clinical imaging biomarker for early bevacizumab treatment response in recurrent GBM1Brain Tumor Imaging Laboratory (BTIL), Center of Computer Vision and Imaging Biomarker, David Geffen School of Medicine, University of California, Los Angeles, Los Angeles, CA, United States, 2Department of Bioengineering, Henry Samueli School of Engineering and Applied Science, University of California, Los Angeles, Los Angeles, CA, United States, 3Department of Radiological Sciences, David Geffen School of Medicine, University of California, Los Angeles, Los Angeles, CA, United States, 4Department of Chemistry and Biochemistry, University of California, Los Angeles, Los Angeles, CA, United States, 5Department of Neurosurgery, David Geffen School of Medicine, University of California, Los Angeles, Los Angeles, CA, United States, 6UCLA Brain Research Institute (BRI), David Geffen School of Medicine, University of California, Los Angeles, Los Angeles, CA, United States, 7Department of Neurology, David Geffen School of Medicine, University of California, Los Angeles, Los Angeles, CA, United States, 8Physics and Biology in Medicine, David Geffen School of Medicine, University of California, Los Angeles, Los Angeles, CA, United States, 9Department of Psychiatry and Biobehavioral Sciences, David Geffen School of Medicine, University of California, Los Angeles, Los Angeles, CA, United States
Synopsis
In the current study we used amine CEST-EPI, a pH-sensitive fast chemical exchange saturation transfer (CEST) technique, as a potential non-invasive imaging biomarker for treatment response in recurrent GBM patients treated with bevacizumab. Results suggest a significantly lower MTRasym at 3.0ppm in recurrent GBM tumors after bevacizumab treatment may be associated with better patient outcome (PFS), indicating that pH-weighted amine CEST MRI could serve as a potential non-invasive imaging biomarker for treatment response evaluation. The colocalization of recurrence tumor site and high MTRasym contrast post-treatment further suggest pH-weighted amine CEST may provide valuable information for early detection of tumor progression.
INTRODUCTION
Glioblastoma (GBM) is an aggressive form of brain tumor with median overall survival (OS) around 15 months despite the intensive therapy, including gross surgical resection followed by radiation therapy and concurrent chemotherapy1. Bevacizumab, a monoclonal antibody against vascular endothelial growth factor (VEGF) that targets angiogenesis, was approved by the Food and Drug Administration for the treatment of recurrent GBM in 2009 based on the ability to improve progression-free survival (PFS); however, subsequent studies have not demonstrated an OS benefit2. Regardless, bevacizumab remains one of the most widely used therapies for recurrent GBM and almost all patients with GBM are exposed to bevacizumab at some time during their treatment.
Tumor angiogenesis is a characteristic feature of malignant transformation. The vasculature of GBM is tortuous, disorganized, and highly permeable3. The malfunction of tumor vasculature and frequent microvascular thromboses promotes intratumoral hypoxia and decreases extracellular pH4. Apart from vessel malfunction and hypoxia, enhanced metabolism and shifted glucose utilization toward glycolysis (i.e. the Warburg effect) also contributes to tumor acidosis5. Imaging biomarkers sensitive to extracellular pH changes may provide a noninvasive measure of metabolism, potentially predicting early treatment response and therapeutic benefit. In the current study we used amine CEST-EPI, a fast chemical exchange saturation transfer (CEST) technique that has been shown to have increased contrast with increasing amino acid concentration and decreasing pH6, as a potential non-invasive imaging biomarker for treatment response in recurrent GBM patients treated with bevacizumab.
METHODS
Patient: A total of 8 males and 3 females recurrent GBM patients from the ages of 45 to 75 years old undergoing bevacizumab treatment were scanned with CEST MRI before and after treatment in the current pilot study. Amine CEST-EPI: Amine CEST-EPI was collected on Siemens 3T scanner (Prisma/Skyra) with previously described CEST-EPI sequence6 or CEST-SAGE-EPI sequence7. Off-resonance saturation was applied using a pulse train of 3x100ms Gaussian pulses with peak amplitude of 6µT. The saturation pulses excite amine protons which resonate at 3.0ppm with respect to water proton frequency. The amine proton exchanges with water proton pool based on a base-catalyzed exchange rate, transferring the saturation effect to water proton signal, which results in the pH-sensitivity of CEST signal. We calculated the magnetization transfer ratio asymmetry (MTRasym) at amine proton resonance frequency (3.0ppm) as the metric of CEST contrast. Data Analysis: The T2 hyperintense lesion (T2 lesion) and contrast enhancing lesion (CE lesion) regions of interest (ROIs) were semi-manually defined as previously described8. A paired t-test was used to evaluate the difference in MTRasym before and after bevacizumab treatment. Spearman’s rank correlation test was performed to evaluate the correlation between MTRasym response and volume response, as well as between MRI metrics and patient outcome (PFS and OS).RESULTS
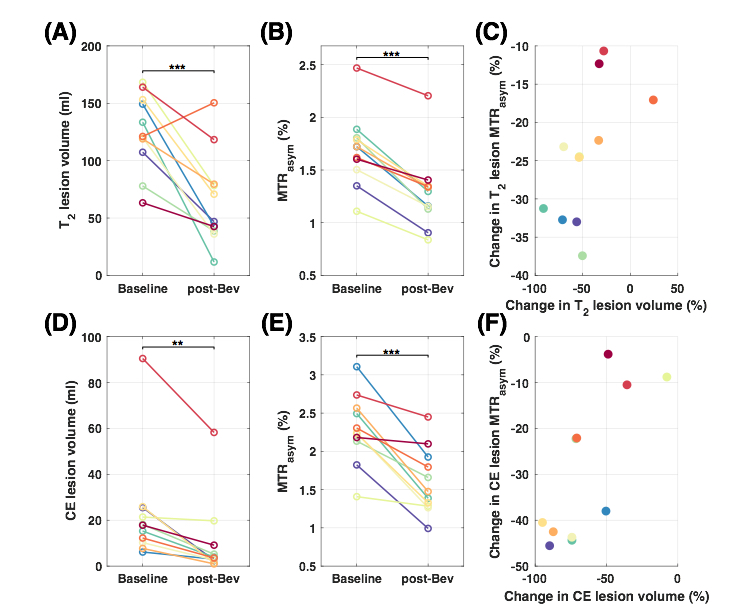
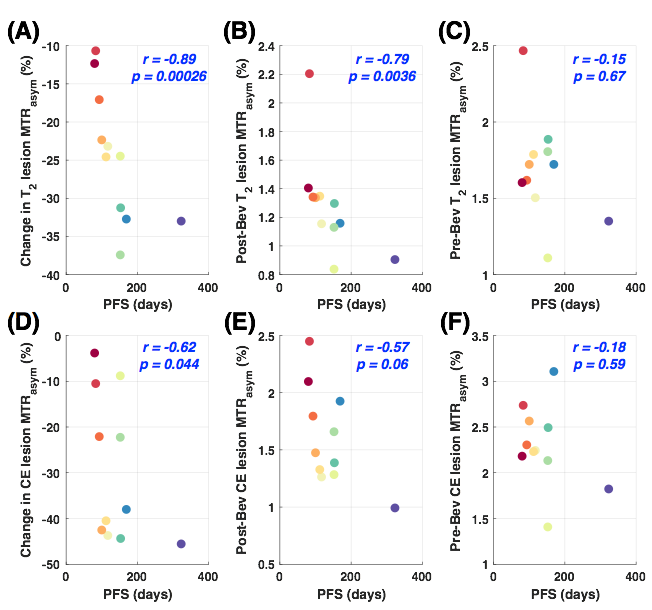
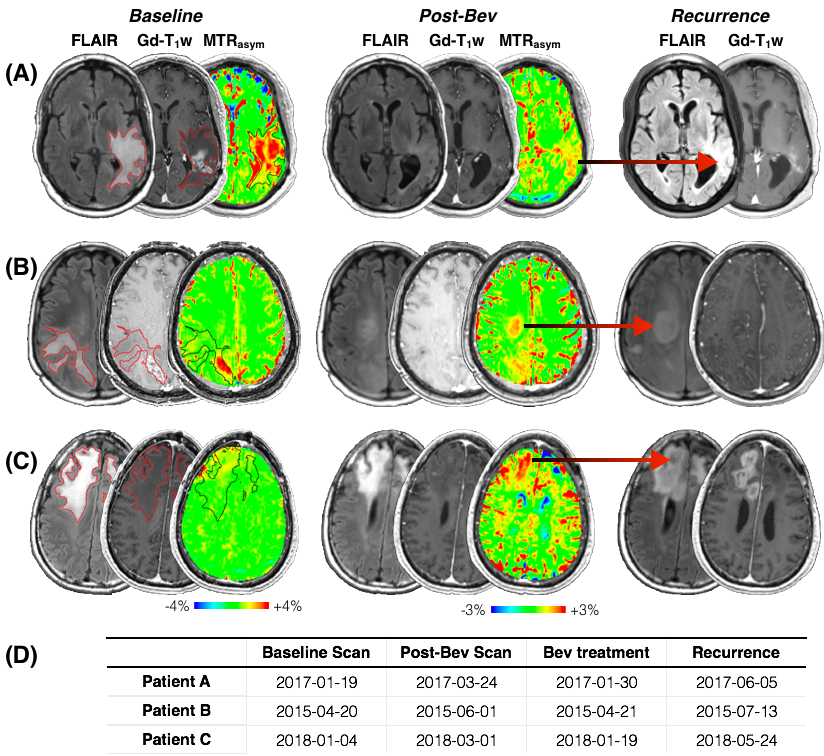
Consistent with previous reports9, we observed dramatic decrease in T2 lesion and CE lesion volumes after bevacizumab treatment (T2 lesion: p=0.00094; CE lesion: p=0.0014; Figure 1(A,D)). MTRasym at 3.0ppm was also significantly lower in post-treatment lesions (T2 lesion: p=5.4e-6; CE lesion: p=0.00022; Figure 1(B,E)). The percentage change in MTRasym was strongly correlated with the percentage change in tumor volume (T2 lesion: r=0.67, p=0.028; CE lesion: r=0.82, p=0.0037; Figure 1(C,F)). Change in MTRasym was negatively correlated with PFS, both in the T2 lesion (r=-0.89, p=0.00026, Figure 2 (A)) and the CE lesion (r=-0.62, p=0.044, Figure 2 (D)). Post-treatment MTRasym in the T2 lesion was also negatively correlated with PFS (r=-0.79, p=0.0036, Figure 2 (B)), although the correlation is was not significant when evaluating MTRasym in the CE lesion (r=-0.57, p=0.060, Figure 2 (E)). No significant correlation was found between pre-treatment MTRasym and PFS, nor between any MTRasym features and OS. We did not find any correlation between volume responses and patient outcome (PFS and OS) in this small cohort. In addition, we observed that in some patients, the site of residue or new emergence of high MTRasym contrast was colocalized with recurrence tumor location, about two months before the recurrent tumor was first observed on conventional MR images (Figure 3).DISCUSSION AND CONCLUSION
Results suggest a significantly lower MTRasym at 3.0ppm in recurrent GBM tumors after bevacizumab treatment may be associated with better patient outcome (PFS), indicating that pH-weighted amine CEST MRI could serve as a potential non-invasive imaging biomarker for treatment response evaluation. The colocalization of recurrence tumor site and high MTRasym contrast post-treatment further suggest pH-weighted amine CEST may provide valuable information for early detection of tumor progression.Acknowledgements
No acknowledgement found.References
1. Stupp R, Mason WP, van den Bent MJ, Weller M, Fisher B, Taphoorn MJ, et al. Radiotherapy plus concomitant and adjuvant Temozolomide for glioblastoma. N Engl J Med. 2005;352:987–96.
2. Chinot OL, Wick W, Mason W, Henriksson R, Saran F, Nishikawa R, Carpentier AF, Hoang-Xuan K, Kavan P, Cernea D, Brandes AA. Bevacizumab plus radiotherapy–temozolomide for newly diagnosed glioblastoma. New England Journal of Medicine. 2014 Feb 20;370(8):709-22.
3. Plate KH, Mennel HD. Vascular morphology and angiogenesis in glial tumors. Experimental and Toxicologic Pathology. 1995 Jan 1;47(2-3):89-94.
4. Rong Y, Durden DL, Van Meir EG, Brat DJ. ‘Pseudopalisading’necrosis in glioblastoma: a familiar morphologic feature that links vascular pathology, hypoxia, and angiogenesis. Journal of Neuropathology & Experimental Neurology. 2006 Jun 1;65(6):529-39.
5. Kato Y, Ozawa S, Miyamoto C, Maehata Y, Suzuki A, Maeda T, Baba Y. Acidic extracellular microenvironment and cancer. Cancer cell international. 2013 Dec;13(1):89.
6. Harris RJ, Cloughesy TF, Liau LM, Prins RM, Antonios JP, Li D, Yong WH, Pope WB, Lai A, Nghiemphu PL, Ellingson BM. pH-weighted molecular imaging of gliomas using amine chemical exchange saturation transfer MRI. Neuro-oncology. 2015 Jun 24;17(11):1514-24.
7. Harris RJ, Yao J, Chakhoyan A, Raymond C, Leu K, Liau LM, Nghiemphu PL, Lai A, Salamon N, Pope WB, Cloughesy TF. Simultaneous p H‐sensitive and oxygen‐sensitive MRI of human gliomas at 3 T using multi‐echo amine proton chemical exchange saturation transfer spin‐and‐gradient echo echo‐planar imaging (CEST‐SAGE‐EPI). Magnetic resonance in medicine. 2018 Apr.
8. Ellingson BM, Kim HJ, Woodworth DC, Pope WB, Cloughesy JN, Harris RJ, Lai A, Nghiemphu PL, Cloughesy TF. Recurrent glioblastoma treated with bevacizumab: contrast-enhanced T1-weighted subtraction maps improve tumor delineation and aid prediction of survival in a multicenter clinical trial. Radiology. 2013 Nov 27;271(1):200-10.
9. Ellingson BM, Cloughesy TF, Lai A, Nghiemphu PL, Mischel PS, Pope WB. Quantitative volumetric analysis of conventional MRI response in recurrent glioblastoma treated with bevacizumab. Neuro-oncology. 2011 Feb 15;13(4):401-9.
Figures