2893
Examining Automatic Segmentation Results of Cervical Spinal Cord MRI in Tetraplegic Spinal Cord InjuryPatrik O Wyss1,2,3, Mihael Abramovic1, Alexander Fischer4, and Markus F Berger1
1Department of Radiology, Swiss Paraplegic Centre, Nottwil, Switzerland, 2Institute for Biomedical Engineering, ETH and University of Zurich, Zurich, Switzerland, 3Max-Planck Institute for Biological Cybernetics, Tuebingen, Germany, 4Philips GmbH Innovative Technologies, Aachen, Germany
Synopsis
Accurate detection and segmentation of spinal levels are of utmost importance in determining tissue changes in follow-up examinations of spinal cord injury patients. This preliminary study shows the results of automatic segmentation algorithms applied to data of tetraplegic patients.
Introduction
Spinal Cord Injury (SCI) is a devastating injury affecting the central nervous system. Accurate detection and segmentation of (pre and post-operative) spinal cord tissue is of high importance in assessing primary spinal cord lesions and secondary tissue damage in spinal cord injury (SCI) and a prerequisite for longitudinal follow-up procedures. In multiple sclerosis (MS) patients, an automatic segmentation of the spinal cord and MS lesions has been published recently1 using convolutional neural networks. The aim of this preliminary study is to assess the automatic level-wise spinal cord segmentation in spinal cord injury.Methods
The dataset includes ten chronic spinal cord injury patients. Images were acquired on a 3T system (Philips Achieva, Best, The Netherlands) using a 3D T2-weighted sequence. Segmentation and data processing was done using IntelliSpace Discovery (Philips, Best, The Netherlands). Manual spinal level segmentation was performed by an experienced radiological technician (MA, 23 years of experience) and reviewed by a radiologist (MFB, 28 years of experience) until consensus was achieved. Automatic segmentation was done using two segmentation algorithms offered by the spinal cord toolbox2: PropSeg3 and DeepSeg1. Pairwise comparison of the segmentation results of the manual and automatic results is done by calculating the Dice Similarity Coefficient (DSC)4. The manual segmentation is regarded as gold standard. Boxplots show the median and quartiles of the DSC of all spinal levels for the comparison of 1) manual vs PropSeg 2) manual vs DeepSeg and 3) DeepSeg vs PropSeg.Results
The demographics of the study participants is shown in Fig.1. We included seven male and three female tetraplegic patients (age: median=57.3 years, range: 28.8-74.7, years since injury: median=16.4 years, range: 1.3-53.5 years), five with complete and five with incomplete tetraplegia. The algorithms provided segmentation results in 9/10 (propSeg) and 8/10 (deepSeg) patients. Fig. 2, 3 and 4 show the segmentation results in patient cases presenting the advantage and pitfalls of automatic segmentation application in tetraplegic spinal cord injury patients. Fig.5 shows the boxplot of the DSC for the three comparisons of all spinal levels where segmentation was possible. Not surprisingly, there is a "dip" of the DSC between C4 and C7, the areas affected by the injury.Discussion
The main findings of this preliminary studies are that automatic segmentation results in spinal cord injury can evoke three scenarios: 1) Although lesion site affects the image quality, both algorithms results in meaningful labelling (Fig.2). 2) Both algorithms perform well in the unaffected levels, but struggle at the lesion site (Fig.3). 3) Automatic segmentation fails because the starting point is wrongly chosen by the algorithm leading to incorrect following levels (Fig.4). Future studies might include a larger number of subjects to train a convolutional neural network to better assess the injury site.Conclusion
This study presents preliminary data of automatic spinal levels segmentation using the spinal cord toolbox in tetraplegic spinal cord injury patients. It is a promising tool for future applications and has great potential for longitudinal follow-up assessments.Acknowledgements
The authors thank the Swiss Paraplegic Foundation for support and J.Cohen-Adad and his group developing the spinal cord toolbox for providing the segmentation routines.References
[1] Gros C et al. Neuroimage 2018; 184:901-915.
[2] De Leener B et al Neuroimage 2017; 145 (Pt A):24-43.
[3] De Leener B et al. Neuroimage 2014; 98:528-536.
[4] Dice LR. Measures of the amount of ecologic association between species. Ecology 1945; 26(3):297-302.
Figures
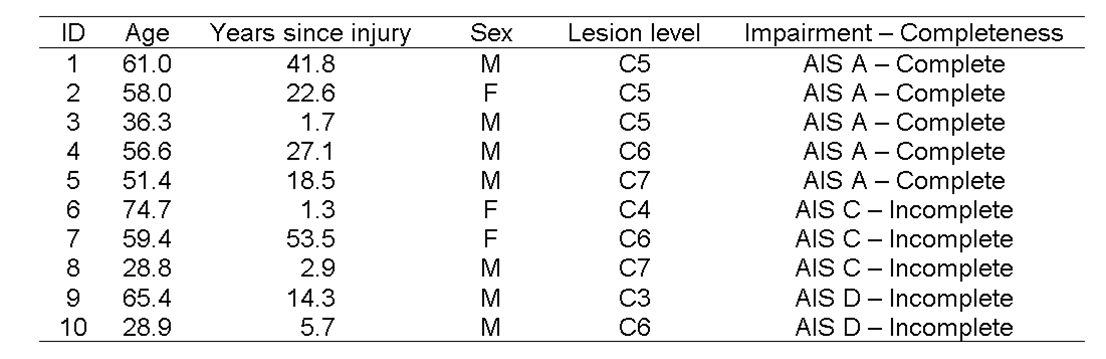
Fig.1:
Dataset demographics of this study including the age, the years since injury, the sex, the lesion level and the
spinal cord injury classification (complete/incomplete).
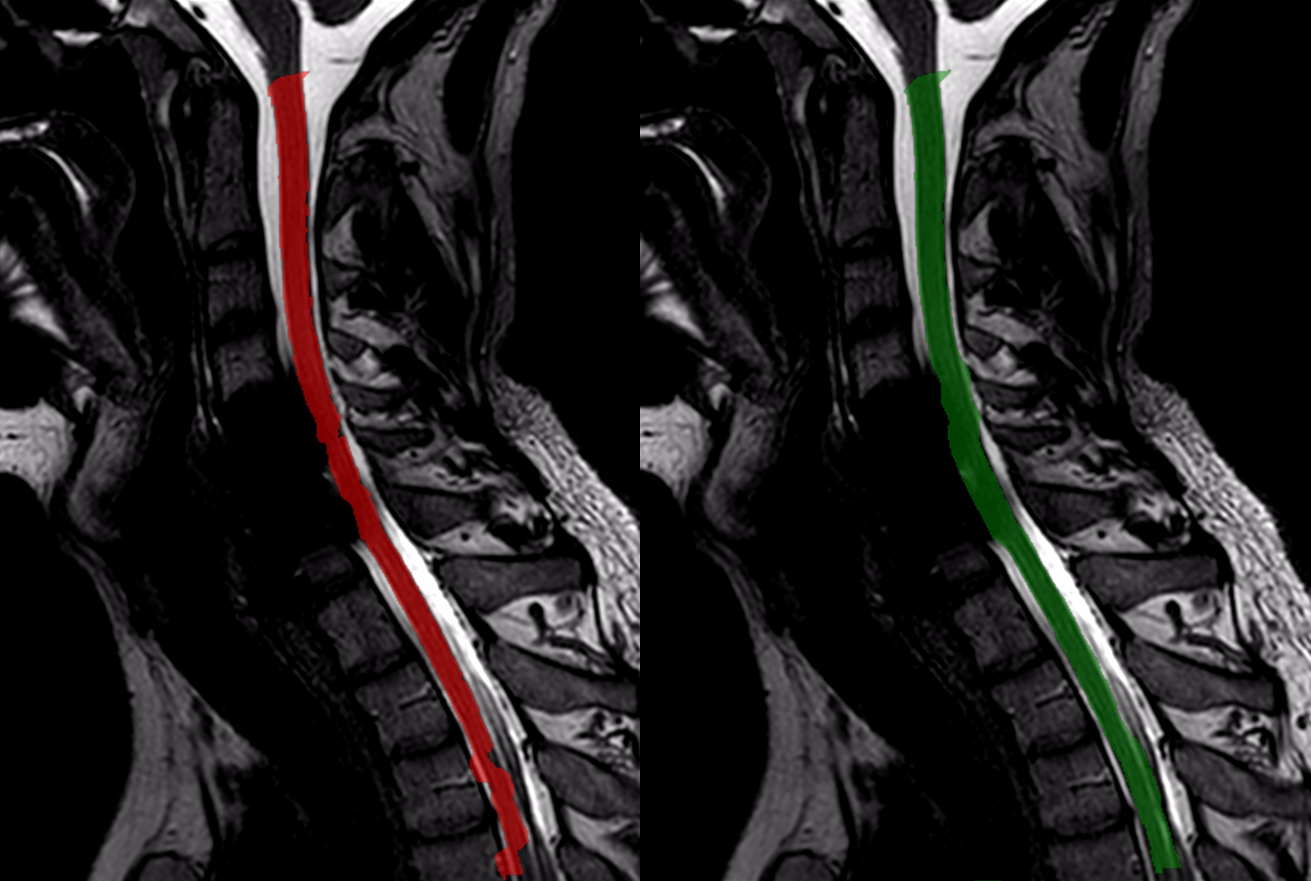
Fig.2: Comparison of the segmentation results of the DeepSeg (left) and
PropSeg (right) algorithms in the same
tetraplegic patient with incomplete SCI
(lesion level: C6).

Fig.3:
Results of the PropSeg (green) in the unaffected levels of a
spinal cord injury patients.
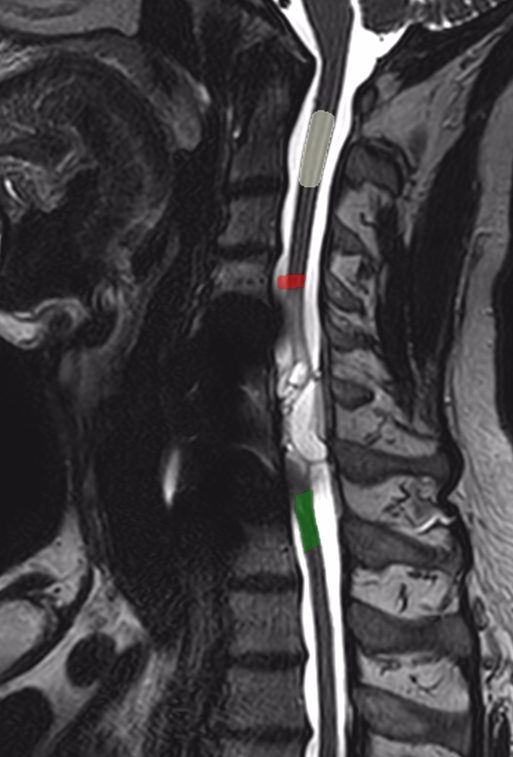
Fig.4:
Results of the DeepSeg (red), PropSeg (green) and
manual segmentation (white) for
the
spinal cord level C2.
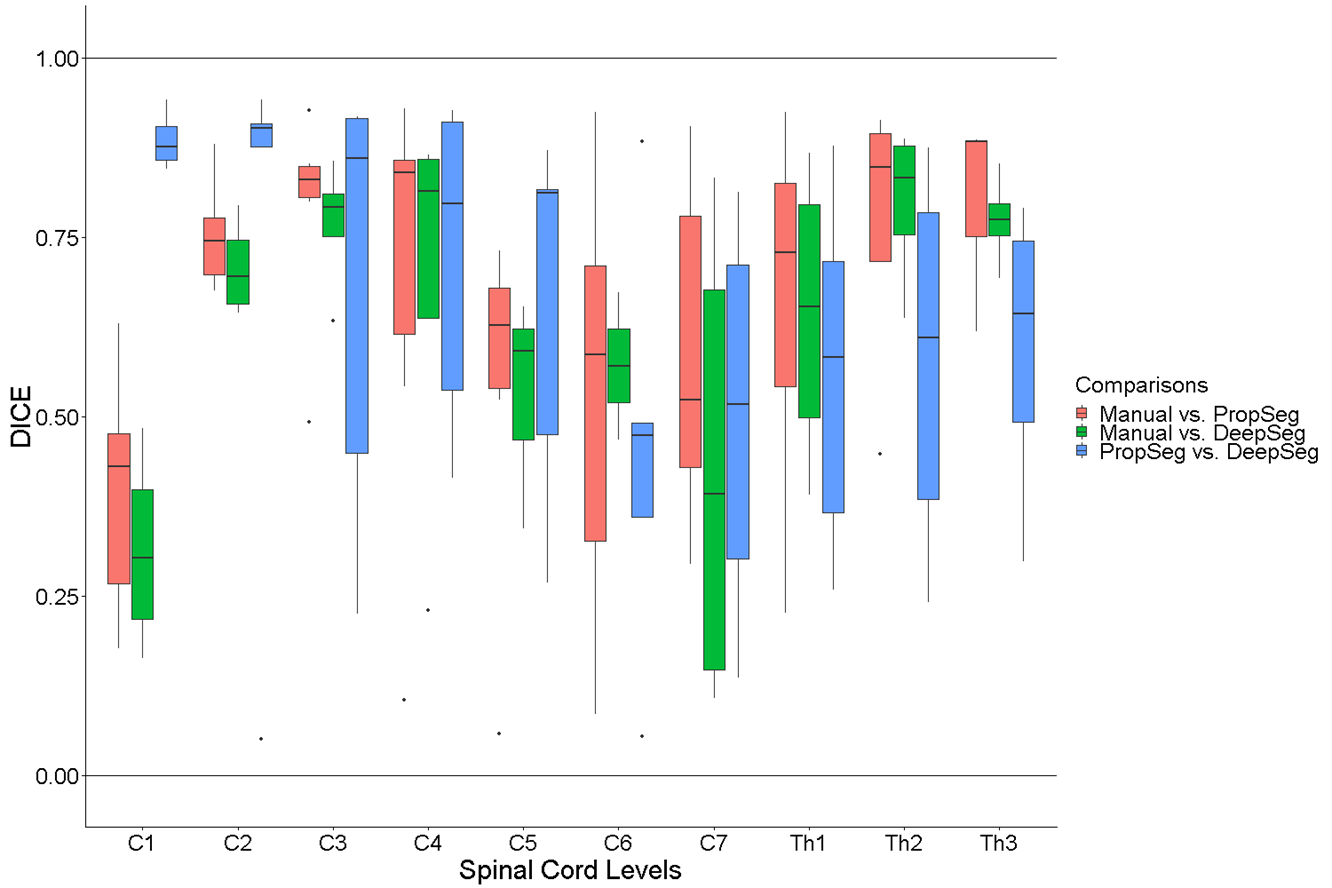
Fig.5:
Boxplot of the Dice similarity coefficient
(DSC) for all spinal levels in all patients where
non-zero values are available. The
DSC is shown for the comparison of 1) manual vs. propSeg (red),
2) manual vs. deepSeg (green) and
3) propSeg vs. deepSeg (blue).