2892
High-resolution Brachial Plexus Imaging using 3-D Short Tau Inversion Recovery (CUBE-STIR) with IV Gadolinium for Vascular Suppression1Radiology and Imaging, Hospital for Special Surgery, New York, NY, United States, 2GE Healthcare, New York, NY, United States, 3Healthcare Research Institute, Hospital for Special Surgery, New York, NY, United States, 4Weill Cornell Medical College, New York, NY, United States
Synopsis
Vascular suppression is critical to facilitate confident identification and pathologic changes of small caliber peripheral nerves, many of great clinical importance, that run alongside slow-flowing veins. In our experience, non-contrast flow suppression techniques are suboptimal for complete venous suppression. Previous studies describe the efficacy of intravenous gadolinium for vascular suppression and visualization of the plexus proper using a three-dimensional STIR pulse, but its use for visualizing small plexus branch nerves has not been reported. This study demonstrated that post-STIR imaging significantly improved vascular suppression and visualization of branch nerves compared to non-contrast techniques, with high inter- and intra-rater agreement.
Disclosures
Disclosures: Dr. Sneag has an institutional research agreement in place with GE Healthcare.Target Audience
Radiologists, PhysicistsIntroduction
MRI plays an important role in diagnosing peripheral neuropathies.1-4 In our experience, conventional, T2-weighted Dixon or short tau inversion recovery (STIR) techniques facilitate reliable identification of the brachial plexus proper (i.e. roots to cords). However, commonly pathologic pre-terminal and terminal branch nerves arising from the plexus can be difficult to confidently visualize due to adjacent vasculature.5
Previous
reports describe the efficacy of intravenous gadolinium (IV-gad) for vascular
suppression and visualization of the plexus proper using a three-dimensional
(3-D) STIR pulse.6,7 Our aim was to determine the utility of 3-D STIR with
IV-gad (‘post-STIR’) to evaluate branch nerves and compare its efficacy to a
3-D, 2-point Dixon sequence (CUBE-Flex) with motion-sensitized driven
equilibrium (MSDE), our current vascular suppression technique.8 We
hypothesized that post-STIR imaging would optimize vascular suppression for
nerve visualization.
Methods
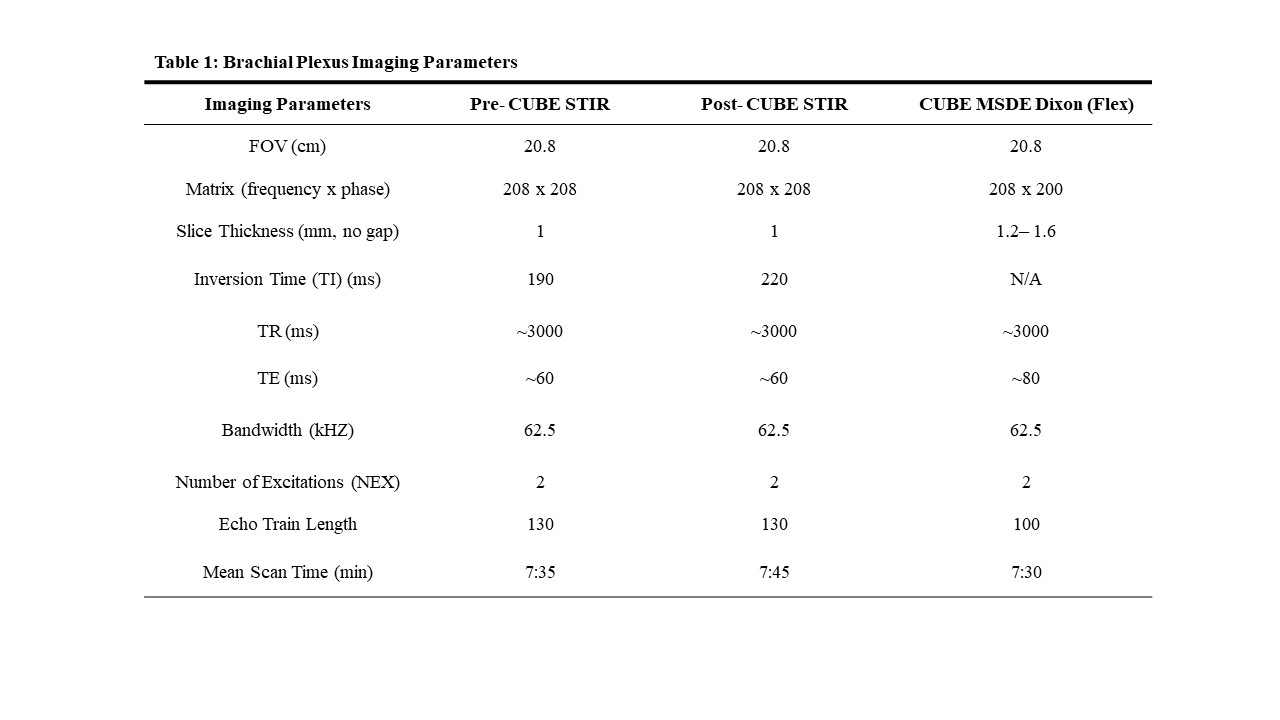
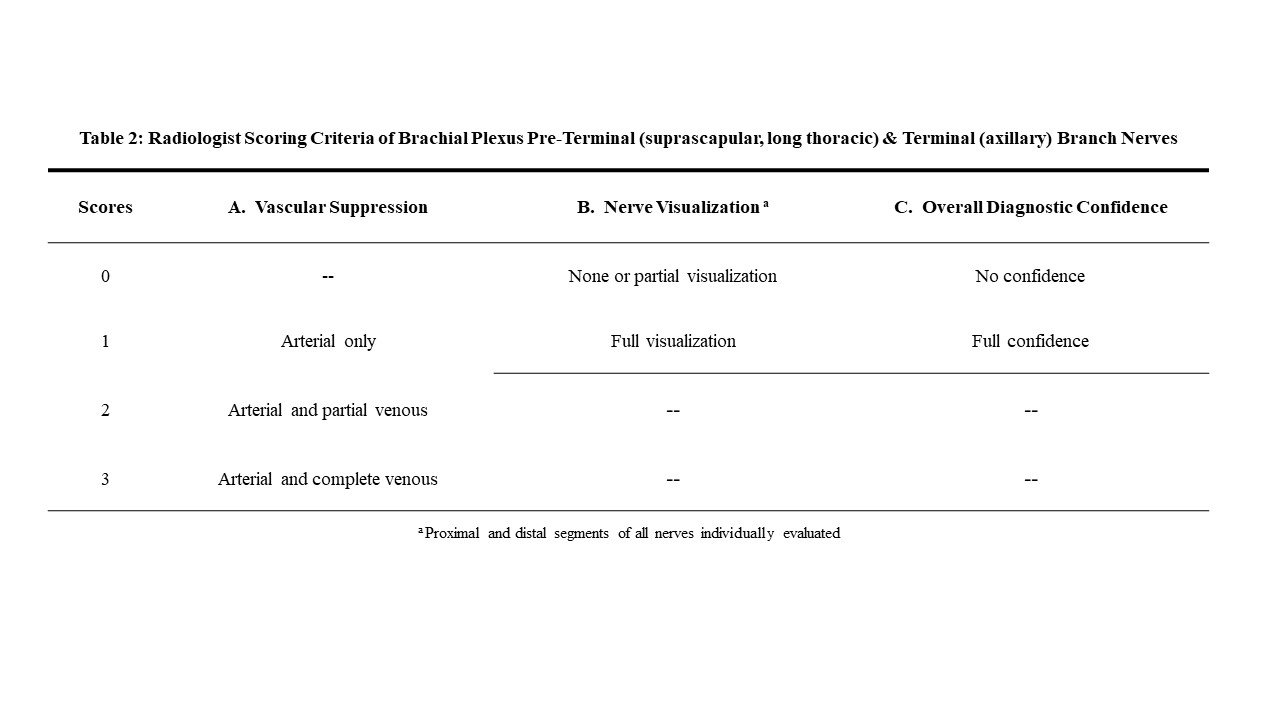
This IRB-approved, prospective study included 28 patients undergoing routine plexus MRI between December 2017 and August 2018. Exams were performed on 3.0T (Discovery MR750, GE Healthcare) using two 16-channel flexible coils. Patients underwent post-STIR (n=28), pre-contrast STIR (‘pre-STIR’) (n=14), and/or pre-contrast MSDE (n=18) imaging, at the radiologist’s discretion (See Table 1 for pulse sequence parameters.) Post-STIR imaging was performed approximately 5 minutes after intravenous Gadovist administration (0.1 mL/kg body weight; 5 mL/s maximum flow rate). Two radiologists (DBS and SD) independently rated blinded sequences (See Table 2 for standardized scoring criteria.) Marginal logistic regression models compared subjective ratings between sequences. Odds ratios (OR) comparing post- to pre-STIR and MSDE were estimated. Inter- and intra-observer agreement was assessed using Gwet’s agreement coefficient (AC; range -1.0–1.0 with 1.0 indicating perfect agreement).Results
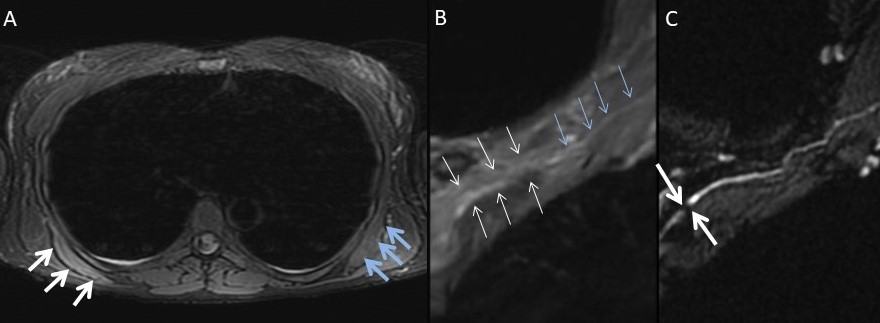
Post-STIR imaging improved vascular suppression (ORMSDE=24.2, 95% CI: 6.9–85, p<0.001; ORPRE=52.6, 95% CI: 8.4–329.0, p<0.001). For all nerves, post-STIR increased diagnostic confidence (ORMSDE=17.4, 95% CI: 7.0–43.3, p<0.001; ORPRE=5.6, 95% CI: 1.5–20.4, p=0.010). Post-STIR also improved nerve visualization (ORMSDE=7.3, 95% CI: 2.8–18.7, p<0.001; ORPRE=4.7, 95% CI: 1.7–12.9, p=0.003), especially for the suprascapular nerve distal segment (ORMSDE=14.8, 95% CI: 3.4–65.3, p<0.001; ORPRE =23.2, CI: 4.5–121.2, p<0.001).
Inter-rater agreement for vascular suppression was almost
perfect (ACMSDE=1, ACPRE=0.92, ACPOST=0.9) and for nerve visualization and
diagnostic confidence moderate to almost perfect in the post-STIR group (AC:
0.41–1.0). Intra-rater agreement for all
criteria post-STIR was similarly high (AC: 0.72–1). Mean scan time was
comparable among all sequences.
Discussion
Post-STIR imaging significantly improved vascular suppression and particularly signal arising from small caliber, slow-flowing veins. Post-STIR imaging also improved visualization of all nerves compared to MSDE and pre-STIR, with high inter- and intra-rater agreement. The most dramatic post-STIR effect was improved visualization of the distal segment of the suprascapular nerve, which innervates critical rotator cuff muscles (supraspinatus, infraspinatus) and is commonly involved in inflammatory and traumatic neuropathies.
STIR employs a recovery pulse with short inversion time (TI ~180-220 ms at 3.0T) to suppress fat at its null point. IV-gad causes shortening of blood’s T1 signal as it approaches the T1 of fat, allowing it to be simultaneously suppressed with the IR pulse (Fig. 1). In our experience, maximal vascular suppression occurs ~6-8 min. following IV-gad, and thus T1-weighted imaging can be obtained with the same contrast bolus.
Limitations of this study include variance in fat suppression techniques (STIR vs. Dixon) and acquired spatial resolution of MSDE and STIR, although our goal was to compare with our standard of care MSDE sequence. Strengths include the application of a clinical cohort, all scanned with the same magnet and surface coils.
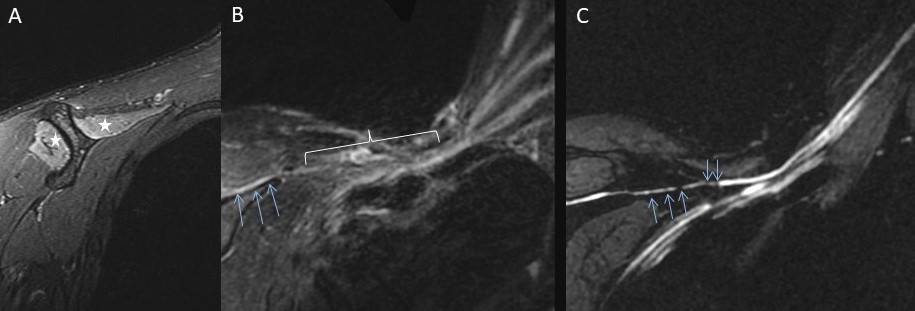
We have since adopted post-STIR imaging in our plexus protocol for select clinical pathologies. In particular, we have found the technique helpful in identifying intrinsic nerve constrictions (Figs. 2-3), a hallmark pathologic finding in neuralgic amyotrophy, which is a syndrome that causes severe weakness in otherwise healthy individuals.9,10
Acknowledgements
No acknowledgement found.References
1. Kwee RM, Chhabra A, Wang KC, et al. Accuracy of MRI in Diagnosing Peripheral Nerve Disease: A Systematic Review of the Literature. AJR Am J Roentgenol. 2014;203(6):1303– 1309.
2. Bäumer P, Pham M, Ruetters M, et al. Peripheral Neuropathy: Detection with Diffusion Tensor Imaging. Radiology. 2014;273(1):185–193.
3. Skorpil M, Karlsson M, Nordell A. Peripheral nerve diffusion tensor imaging. Magn Reson Imaging. 2004;22(5):743–745.
4. Thawait SK, Chaudhry V, Thawait GK, et al. High-Resolution MR Neurography of Diffuse Peripheral Nerve Lesions. AJNR Am J Neuroradiol. 2011;32(8):1365–1372.
5. Deshmukh S, Fayad LM, Ahlawat S. MR neurography (MRN) of the long thoracic nerve: retrospective review of clinical findings and imaging results at our institution over 4 years. Skeletal Radiol. 2017;46(11):1531-1540.
6. Chen WC, Tsai YH, Weng HH, et al. Value of enhancement technique in 3D-T2-STIR images of the brachial plexus. J Comput Assist Tomogr. 2014;38(3):335–339.
7. Wang L, Niu Y, Kong X, et al. The application of paramagnetic contrast-based T2 effect to 3D heavily T2W high-resolution MR imaging of the brachial plexus and its branches. Eur J Radiol. 2016;85(3):578-584.
8. Sneag DB, Miyoshi M, Fung M, et al. Peripheral Nerve Imaging using 2-point Dixon 3D Fast Spine Echo (CUBE-FLEX) with Flow-Saturation Preparation (FSP): Initial Feasibility Study. ISMRM 2016 Proceeding P. 2997.
9. Sneag DB, Rancy SK, Wolfe SW, et al. Brachial plexitis or neuritis? MRI features of lesion distribution in Parsonage-Turner syndrome. Muscle Nerve. 2018;58(3):359–366.
10. Sneag DB, Saltzman EB, Meister DW, et al. MRI bullseye sign: An indicator of peripheral nerve constriction in Parsonage-Turner syndrome. Muscle Nerve. 2017;56(1):99–106.
Figures
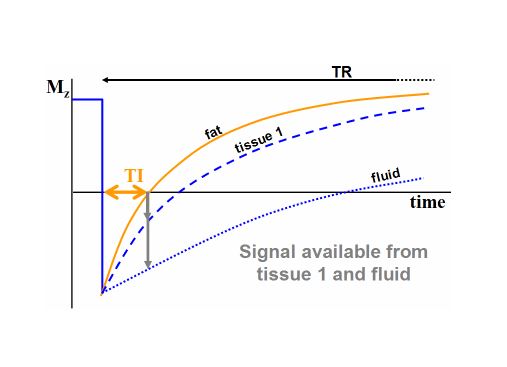
Figure 1: This graphical
illustration demonstrates the effect of IV-gadolinium on the MR signal
evolution of blood. As such, the inversion time of IV-gadolinium doped blood
(tissue 1) approaches that of fat.