2890
Relevance of spinal white matter suppressed T1 STIR beyond multiple sclerosisUllas V Acharya1, Rupesh Vakkachi Kandi2, Narayana Krishna Rolla3, Jitender Saini4, Brian Johnson5, and Jaladhar Neelavalli2
1Radiology, Manipal Hospital, Bengaluru, India, 2Philips Innovation Campus, Philips India Limited, Bengaluru, India, 3Philips India Limited, Gurgaon, India, 4Radiology, National Institute of Mental Health And Neurosciences, Bengaluru, India, 5Philips Healthcare, Dallas, TX, United States
Synopsis
Previous works have shown that white matter suppressed (WMS) T1 STIR imaging can provide better lesion contrast in spine in multiple sclerosis. In this work we have explored the relevance of this technique in non multiple sclerosis related spinal conditions. The results show that, in these conditions as well, T1 STIR provides better lesion conspicuity.
Introduction
Lesions can occur within the spinal cord in various conditions such as demyelination, infection, trauma, tumour, infarction, cord compression etc. Accurate diagnosis is critical for appropriate therapeutic management and clinical outcome. T2 weighted turbo spin echo (T2 TSE) is one of the standard and primary techniques used for lesion assessment in the spinal cord.1,2 In the recent past white matter suppressed (wms) T1 weighted TSE sequence, also referred to as T1 STIR (short tau inversion recovery), has been shown to be better than the conventional sequences in better conspicuity in spinal lesion detection in Multiple sclerosis.3 However, reports on its applicability in non-MS spinal conditions are scant. In this work we have applied wms T1 STIR in cases of spinal conditions other than MS, to explore its relevance in these conditions.Materials and Methods
WMS T1 STIR data was acquired in 4 patients with different spinal conditions – spinal infarction, trauma post infective transverse myelitis and ADEM (acute disseminated encephalomyelitis) (see Table-1 for imaging parameters) in addition to the conventional spine imaging protocol. In one of the patients, with ADEM, data was acquired at two time points, 10 weeks apart – pre-treatment and post-treatment. Another patient, with spinal infarction was also imaged twice – 1 day apart. WMS T1 STIR images were compared with the conventional T2 TSE sagittal and/or T2 TSE axial for the visualization of lesion and artifacts.Results
Figures 1 to 4 compare the visualization of lesions in the cases of infarction, post infective transverse myelitis, ADEM, and spinal trauma respectively. Conspicuity of the lesions was better in WMS T1 STIR compared to the conventional T2 TSE. In the ADEM case, the effect of treatment was more clearly visualized with WMS T1 STIR compared to T2 TSE.Discussion and Conclusion
Use of IR sequence in detecting white matter lesions of brain is well established with sequences developed to suppress CSF like FLAIR as well as white mater in Double IR sequences with 3D acquisitions to better depict various white mater lesions and hence characterize disease burden.1 A good spectrum of such conditions also involve spinal cord; lesions of which have always been a challenge to pick up employing conventional sequences like T2 weighted image owing to acquisition related parameters, artefacts and inter-reader variability in lesion count.4 As gray mater forms a significantly smaller component (by volume) of cord parenchyma, with negligible inherent differentiation between gray and white mater of spinal cord; it seems sufficient to employ a sequence with selective white mater suppression to depict lesions in spine, even in non-MS conditions. Differentiation between various conditions involving cord parenchyma is of extreme clinical importance as management decisions vary impacting clinical outcome. For example, differentiation between a hyperacute condition like spinal cord infarct from more treatable condition like demyelination implies different treatment regimens and prognosis. It is also important to characterize type of lesion for differentiating various demyelinating diseases like MS, NMO and ADEM; treatment of which are quite different and could even potentially worsen existing condition as in NMO if treated with interferon beta which is used to treat MS. Also depiction of lesion response to treatment, development of new lesions can independently influence treatment modifications on follow up. In this context, better conspicuity of lesions, offered by WMS T1 STIR is desirable and could be either used as an adjunct to T2 weighted image or as a standalone sequence. The present study is a preliminary work in exploring the relevance of WMS T1 STIR in non-MS spinal conditions. While the results are promising, application in a larger cohort is warranted for statistically establishing its utility.Acknowledgements
No acknowledgement found.References
1. Americal College of Radiology. ACR–ASNR–SCBT-MR–SSR PRACTICE PARAMETER FOR THE PERFORMANCE OF MAGNETIC RESONANCE IMAGING (MRI) OF THE ADULT SPINE.; 2018. 2. Simon JH, Li D, Traboulsee A, et al. Standardized MR imaging protocol for multiple sclerosis: Consortium of MS Centers consensus guidelines. In: American Journal of Neuroradiology. ; 2006. doi:27/2/455 [pii] 3. Poonawalla AH, Hou P, Nelson FA, Wolinsky JS, Narayana PA. Cervical Spinal Cord Lesions in Multiple Sclerosis: T1-weighted Inversion-Recovery MR Imaging with Phase-Sensitive Reconstruction. Radiology. 2008. doi:10.1148/radiol.2463061900 4. Altay EE, Fisher E, Jones SE, Hara-Cleaver C, Lee JC, Rudick RA. Reliability of classifying multiple sclerosis disease activity using magnetic resonance imaging in a multiple sclerosis clinic. JAMA Neurol. 2013. doi:10.1001/2013.jamaneurol.211Figures

Figure-1: Images of a patient with spinal cord infarct where the lesion is seen
best on WMS corresponding to diffusion restriction, as compared to T2 weighted
image (in Time point 2). In the T2 TSE sequence, acquired in time point 1
(which is closer in time to onset of infarction) the lesion is not visualized
clearly. Unfortunately, WMS T1 STIR was not acquired at time point 1 for
comparison.
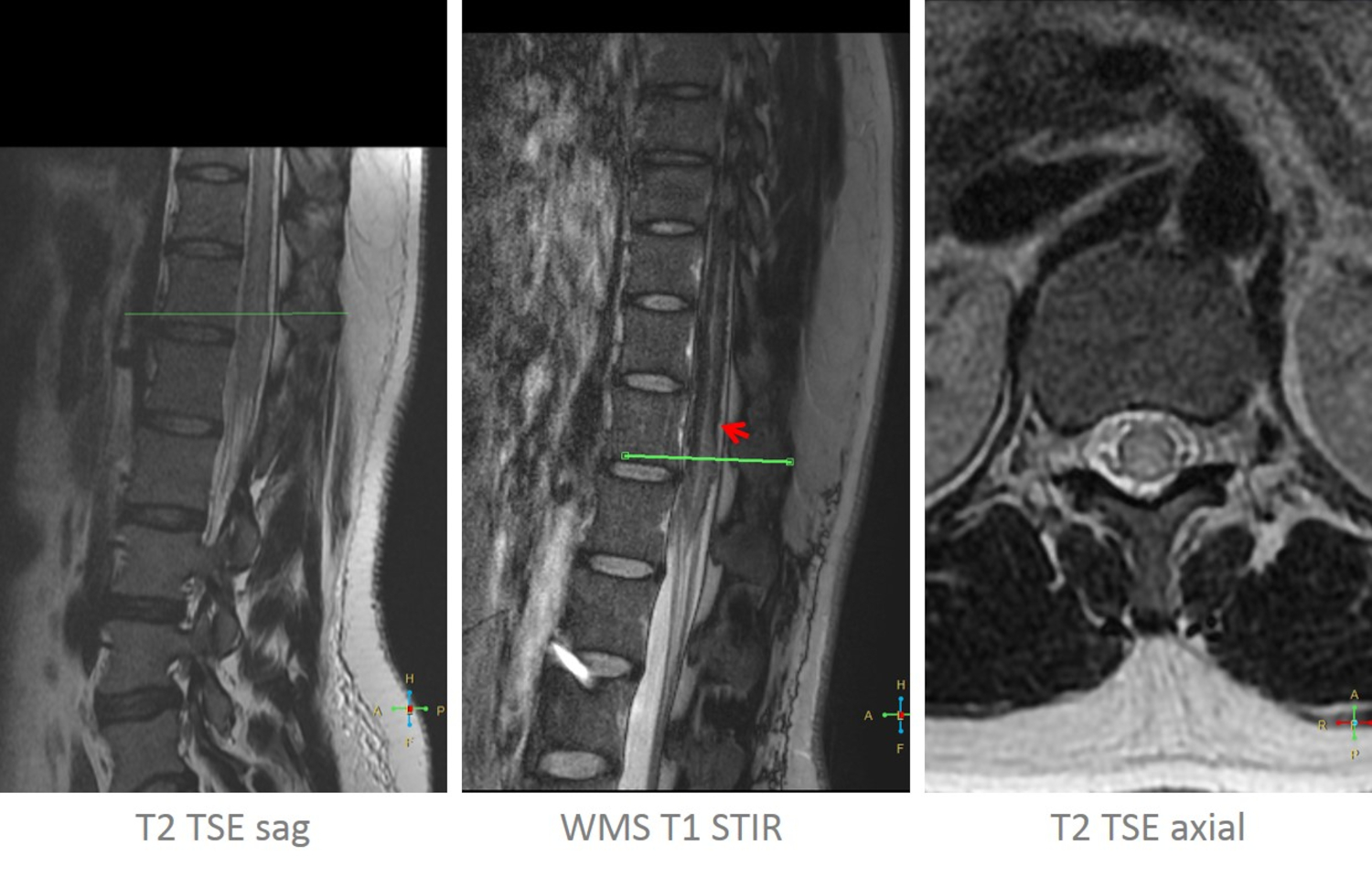
Figure 2: Images of a patient with post
infective transverse myelitis where long segment involvement of the cord is
better depicted on WMS as compared to T2 sequence.

Figure 3: Images of the patient with ADEM
showing decrease in signal intensity and extent of lesion post treatment on
follow up as compared to pre-treatment image best visualized on WMS image.

Figure 4: Images of a patient with spinal cord injury
where the lesion is seen on T2 TSE, WMS T1 STIR and mFFE sequences.
Nevertheless the extent and the boundary of the lesion is appreciated more
clearly in WMS T1 STIR.

Table-1: Sequence parameters