2874
T2 mapping of lumbosacral nerves in patients suffering from unilateral radicular pain due to degenerative disc disease1Department of Diagnostic and Interventional Neuroradiology, Klinikum rechts der Isar, Technische Universität München, Munich, Germany, 2Department of Diagnostic and Interventional Radiology, Klinikum rechts der Isar, Technische Universität München, Munich, Germany, 3Philips Healthcare, Hamburg, Germany, 4Department of Neurosurgery, Klinikum rechts der Isar, Technische Universität München, Munich, Germany
Synopsis
It is long known that findings in conventional anatomical imaging do not necessarily correlate with clinical symptoms in patients suffering from unilateral lumbosacral radicular syndrome (LRS), which regularly occurs in the context of disc herniation due to degeneration with unilateral nerve contact. The present study investigates the performance of quantitative imaging by using magnetic resonance neurography (MRN) using T2 mapping for LRS diagnostics at the lumbosacral plexus. As the main finding, it shows that nerves affected by degenerative disc herniation are characterized by elevated T2 values, in contrast to contralateral nerves or a non-affected control level.
Introduction
Unilateral lumbosacral radicular syndrome (LRS) is a common condition that often leads to diagnostic imaging with the aim of detecting a structural cause when symptoms are longer-lasting. However, findings in conventional anatomical imaging do not necessarily correlate with clinical symptoms. 1,2,4 Imaging is primarily performed for the qualitative evaluation of surrounding, compressing structures like herniated discs instead of evaluations of the nerves directly. The present study investigates the performance of quantitative imaging by using magnetic resonance neurography (MRN) for LRS diagnostics.Methods
Subjects: Eighteen patients (10 males & 8 females; mean age: 64.4 ± 10.2 years) were enrolled, all presenting with strict unilateral LRS matching at least one dermatome and presence of symptoms for at least four weeks and not longer than six months. Previous anatomical imaging indicated disc herniation due to degeneration with unilateral nerve contact of degenerated disc material in all cases.
MRI: MRN was performed using a 3T whole-body scanner (Ingenia, Philips Healthcare, Best, The Netherlands) with a 16-channel torso coil array and a built-in-table posterior 12-channel coil array. The scanning protocol included an adiabatic T2-prepared, three-dimensional (3D) turbo spin echo (TSE) sequence with fat suppression using SPectral Attenuated Inversion Recovery and variable duration of the T2 preparation for the purpose of T2 mapping of LSP nerves with the following sequence parameters: field of view (FOV) = 38×38×8 cm3, acquisition voxel = 2×2×2 mm3, echo train length = 80, T2 preparation durations of 20/40/60/80 ms, repetition time = 1.6 s, echo time of the TSE shot = 15 ms. 3,5 A modified B1-insensitive rotation (BIR-4) pulse was applied for T2 preparation in order to minimize the sensitivity to B0 and B1 inhomogeneities. 3,5 The duration of the sequence was 6 min and 48 s. Furthermore, we acquired a flow-suppressed T2-weighted, 3D TSE sequence with an isotropic voxel size of 2 mm to depict LSP anatomy, with the FOV covering at least the L2 – S2 nerves.
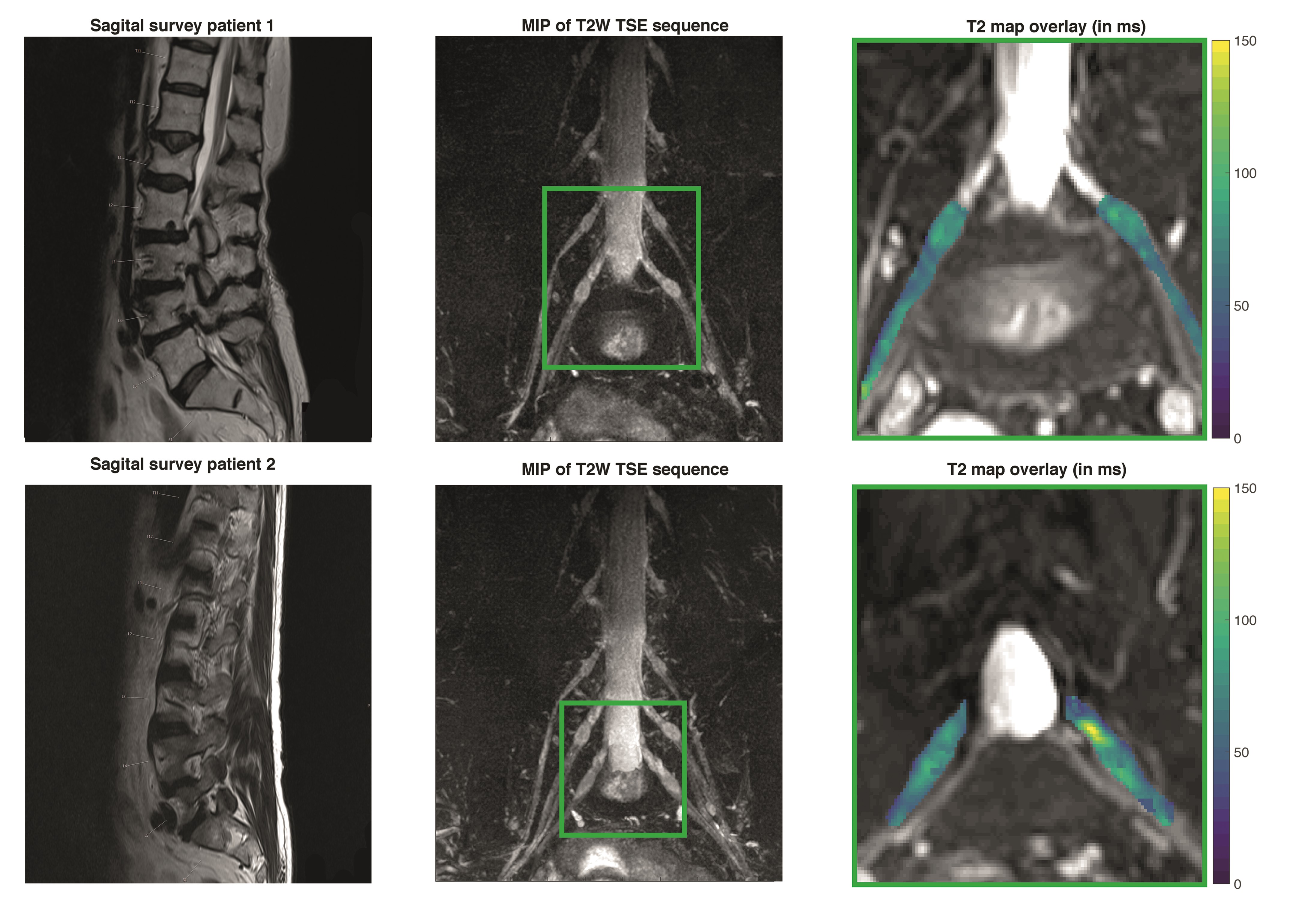
Image analysis: A voxel-by-voxel approach with a combination of golden section search and variable projection (VAPRO) was used to generate T2 maps out of the adiabatic T2-prepared TSE sequence. 5 The obtained maps were uploaded to Horos software (version 1.1.7; https://www.horosproject.org) for quantitative analyses of T2 values of nerves. The investigator was blinded to the side of symptoms, but was informed about the level of suspected nerve contact to degenerated disc material according to previous anatomical imaging. The level of the affected nerve was identified on T2 maps with applied color scheme. Manual placement of polygonal regions of interest (ROIs) in axial slices of the T2 maps was performed for the left and right nerve of the affected level at a preganglionic (~1 cm before the ganglion), ganglionic (in the middle of the ganglion), and postganglionic (~1 cm after the ganglion) site, followed by extracting of T2 values of these ROIs (Fig. 1). 5 As an internal reference, the L2 nerve of both sides (not affected by degenerative disc herniation in any of the patients) was subsequently identified, and preganglionic, ganglionic, and postganglionic ROIs were drawn analogous to the approach at the affected level (Fig. 1). Furthermore, the flow-suppressed T2-weighted TSE sequences were screened qualitatively for T2-hyperintense signal alterations in nerves of the affected level.
Epidural steroid injection (ESI): After MRN, patients underwent unilateral ESI with local anesthetics for diagnostic purposes at the site of suspected nerve affection according to previous anatomical imaging.
Results
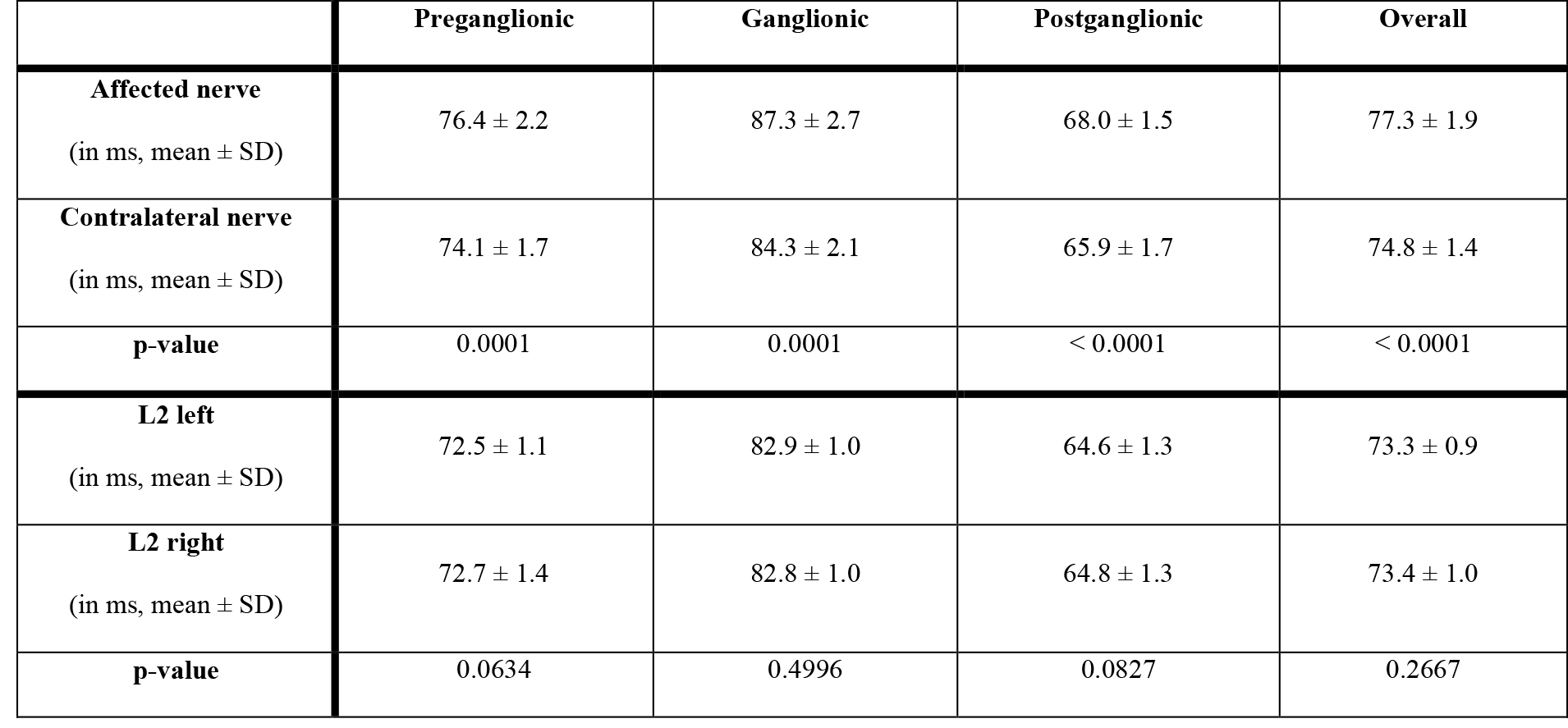
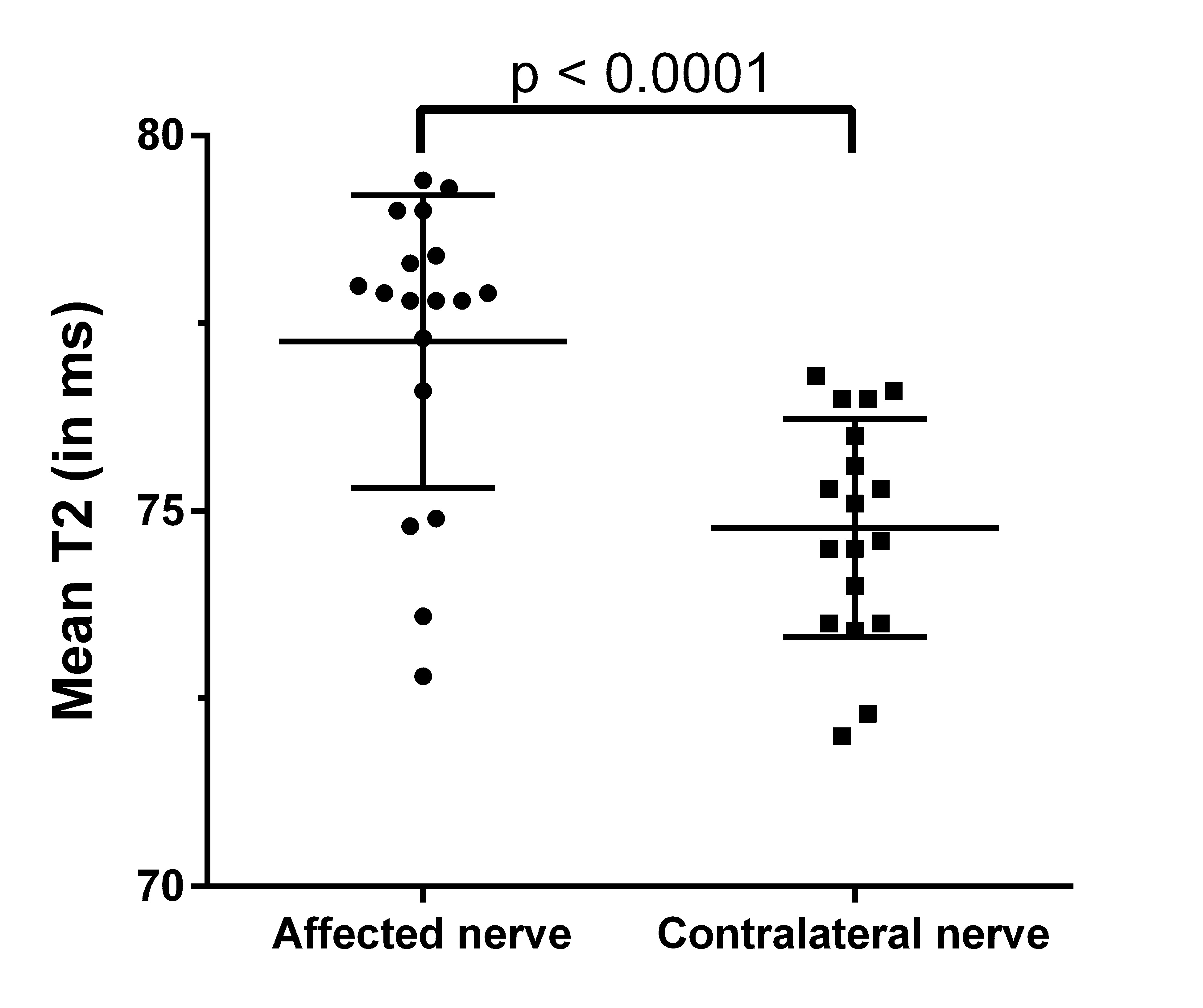
Mean T2 was 77.3 ± 1.9 ms in the affected nerves, whereas it accounted for 74.8 ± 1.4 ms in the contralateral nerves (p < 0.0001; Figs. 2 & 3). Measurements along the left L2 resulted in an average T2 value of 73.3 ± 0.9 ms, and it was 73.4 ± 1.0 ms for the right L2 (p = 0.2667; Figs. 2 & 3). Furthermore, signal alterations in the T2-weighted 3D TSE sequences according to visual inspection were present within the affected nerves in four patients (22.2%), whereas the remaining fourteen patients (78.8%) did not show any clear T2 signal increases within affected nerves. In relation to ESI performed at the site of suspected nerve affection, MRN with T2 mapping had a sensitivity / specificity of 76.9% / 60.0%.Discussion & Conclusion
The present study shows that nerves affected by degenerative disc herniation are characterized by elevated T2 values. Thus, quantitative MRN by means of T2 mapping could be a diagnostically useful add-on technique to anatomical imaging in neurosurgical patients with unilateral LRS, but uncertainty regarding the distinct level causing symptoms (e.g., manifestation of degenerative disc disease at multiple levels).Acknowledgements
This project was partially supported by Philips Healthcare and has received funding from the European Research Council (ERC) under the European Union’s Horizon 2020 research and innovation program (grant agreement No 637164 — iBack — ERC-2014-STG). This work reflects only the authors view and the EU is not responsible for any use that may be made of the information it contains.References
1. Delauche-Cavallier MC, Budet C, Laredo JD, et al. Lumbar disc herniation. Computed tomography scan changes after conservative treatment of nerve root compression. Spine (Phila Pa 1976). 1992;17(8):927-933.
2. Jensen MC, Brant-Zawadzki MN, Obuchowski N, et al. Magnetic resonance imaging of the lumbar spine in people without back pain. N Engl J Med. 1994;331(2):69-73.
3. Klupp E, Weidlich D, Schlaeger S, et al. B1-insensitive T2 mapping of healthy thigh muscles using a T2-prepared 3D TSE sequence. PLoS One. 2017;12(2):e0171337.
4. Maigne JY, Rime B, Deligne B. Computed tomographic follow-up study of forty-eight cases of nonoperatively treated lumbar intervertebral disc herniation. Spine (Phila Pa 1976). 1992;17(9):1071-1074.
5. Sollmann N, Weidlich D, Cervantes B, et al. High Isotropic Resolution T2 Mapping of the Lumbosacral Plexus with T2-Prepared 3D Turbo Spin Echo. Clin Neuroradiol. 2018 [Epub ahead of print].
Figures